


Case from: Bharat Bhooshan Kukreti1, Gurpreet Singh Gulati2, Sivasubramanian Ramakrishnan1, Balram Bhargava1, Sandeep Seth1
Institute: Department of Cardiology1 and Department of Cardiovascular Radiology2, All India Institute of Medical Sciences (AIIMS), New Delhi, India
Clinical history: A 65 year old, non-diabetic, normotensive and obese female complained of exertional angina of four years’ duration. She had a transient ischemic attack 15 days ago. Physical examination was unremarkable.
ECG showed poor precordial R wave progression with q waves in V1-6, II, III and aVF leads, along with T wave inversions in precordial leads. However, patient denied any history suggestive of acute coronary syndrome (Fig. 1).
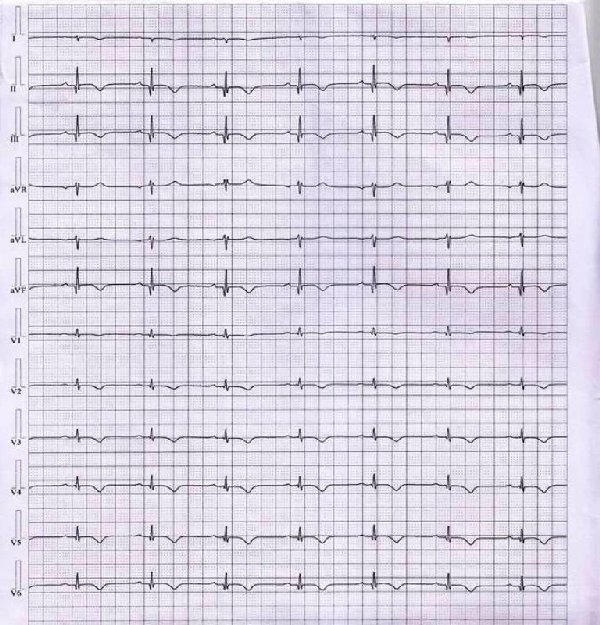
Fig 1.
ECHO showed normal left ventricular (LV) function, dimensions and wall thickness. ECHO window was however, poor for evaluation of LV apex.
Coronary angiography was normal. LV injection revealed a spherical calcified cavity projecting outwards and communicating with the LV apex. The lesion was akinetic and filling partially with contrast, suggestive of mural thrombus. No other regional wall motion abnormality was noted (Fig. 2A & B).
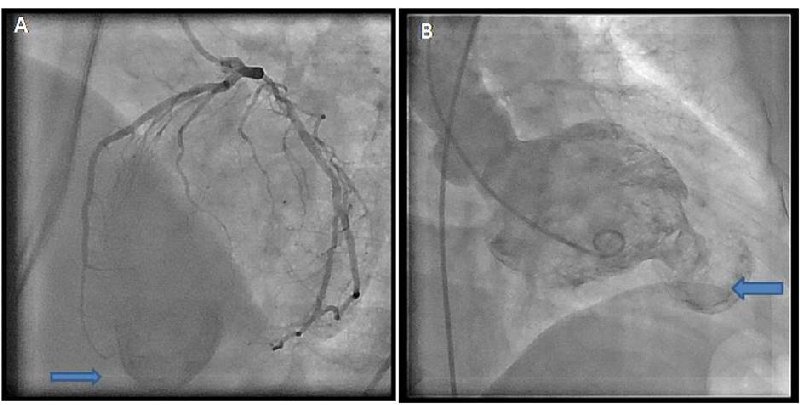
Fig 2A & B
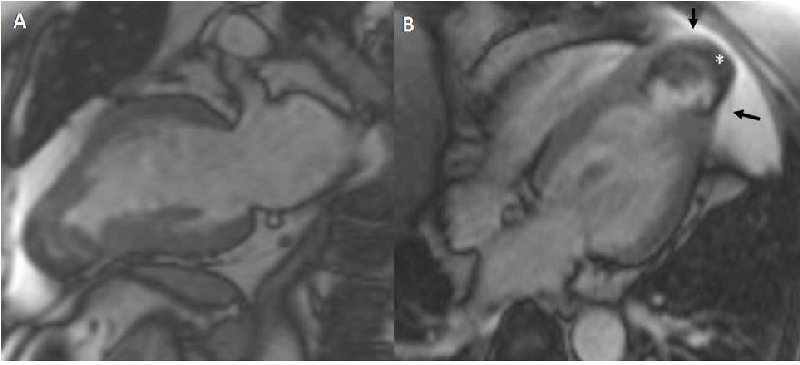
Fig 3A & B
CMR Findings: Cardiac MRI revealed asymmetric hypertrophy of left ventricle (interventricular septum: 14 mm; posterior wall: 10 mm). The septum was more hypertrophied towards the apex. The apical lesion with its neck shared a common myocardium with the left ventricle. The walls of the lesion were calcified (Fig. 3A & B). Delayed enhanced images showed transmural enhancement of the lesion, consistent with fibrosis and confirmed presence of mural thrombus (Fig. 4A & B). Cine images showed normal LV function except for the apical region which was akinetic (movie). The pericardium was intact along the apex. The final diagnosis of apical hypertrophic cardiomyopathy with apical aneurysm was made based upon these cardiac MRI findings. Patient was started on beta blockers and anticoagulation.
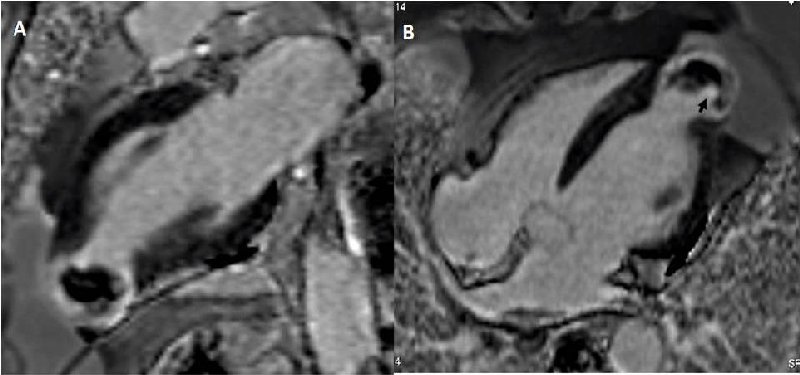
Fig 4A & B
Movie
Conclusion: Apical aneurysm in absence of epicardial coronary artery disease is a rare complication of apical hypertrophic cardiomyopathy. High intra-ventricular pressures, local abnormalities of cardiac contraction and intramural coronary artery abnormalities may produce a chronically ischemic state of apical myocardium and cause aneurysm formation.
References:
1 . Toda G, Iliev II, Kawahara F, Hayano M , Yano K. Left ventricular aneurysm without coronary artery disease, incidence and clinical features: clinical analysis of 11 cases . Intern Med 2000;39:531- 536.
2 . Barbaresi F, Longhini C, Brunazzi C, Caneva M , Cotogni A , Musacci GF , Rigatelli G , Volta G. Idiopathic apical left ventricular aneurysm in hypertrophic cardiomyopathy. Report of 3 cases,and review of the literature. Jpn Heart J 1985; 26:481- 494.
3 . Anon RO, Rosing DR, Maron BJ, Leon MB , Bonow RO , Watson RM , Epstein SE. Myocardial ischemia in patients with hypertrophic cardiomyopathy: contribution of inadequate vasodilator reserve and elevated left ventricular filing pressures. Circulation 1985;71:234- 243.
4 . Tengyong J, Zhihong H, Jing W , Qiang L, Xuesi W. Hypertrophic cardiomyopathy with apical left ventricular aneurysm: a case report Chinese Medical Journal , 2002,115 No. 5: 782-784
COTW handling editor: Vikas K. Rathi, MD
Have your say: What do you think? Latest posts on this topic from the forum


