



Diego Perez de Arenaza, Santiago del Castillo, Marcelo Pietrani, Mariano Falconi, Juan Benger, Ezequiel Levy Yeyati, Luciano Destefano, Ezequiel Guzzetti, Ricardo Garcia Monaco, Arturo Cagide
Hospital Italiano de Buenos Aires, Argentina
Clinical Presentation:
An 81-year-old male patient presented with sudden and intense chest pain. On the emergency ward, a transthoracic echocardiogram was performed showing an enlarged and wall-thickened thoracic aorta. Computed tomography angiography confirmed the enlarged and wall-thickened thoracic aorta. In non-contrast images, a high-attenuation crescentic thickening of the aortic wall suggested an intramural hematoma or aortitis (Figure 1). 18F-FDG-PET suggested that there was no overt inflammation but findings were equivocal (Figure 1). The patient was stable without pericardial effusion, periaortic hematoma, or large aortic aneurysm; therefore, a cardiac magnetic resonance imaging study was performed in the next 12 hours to rule out aortitis (1).
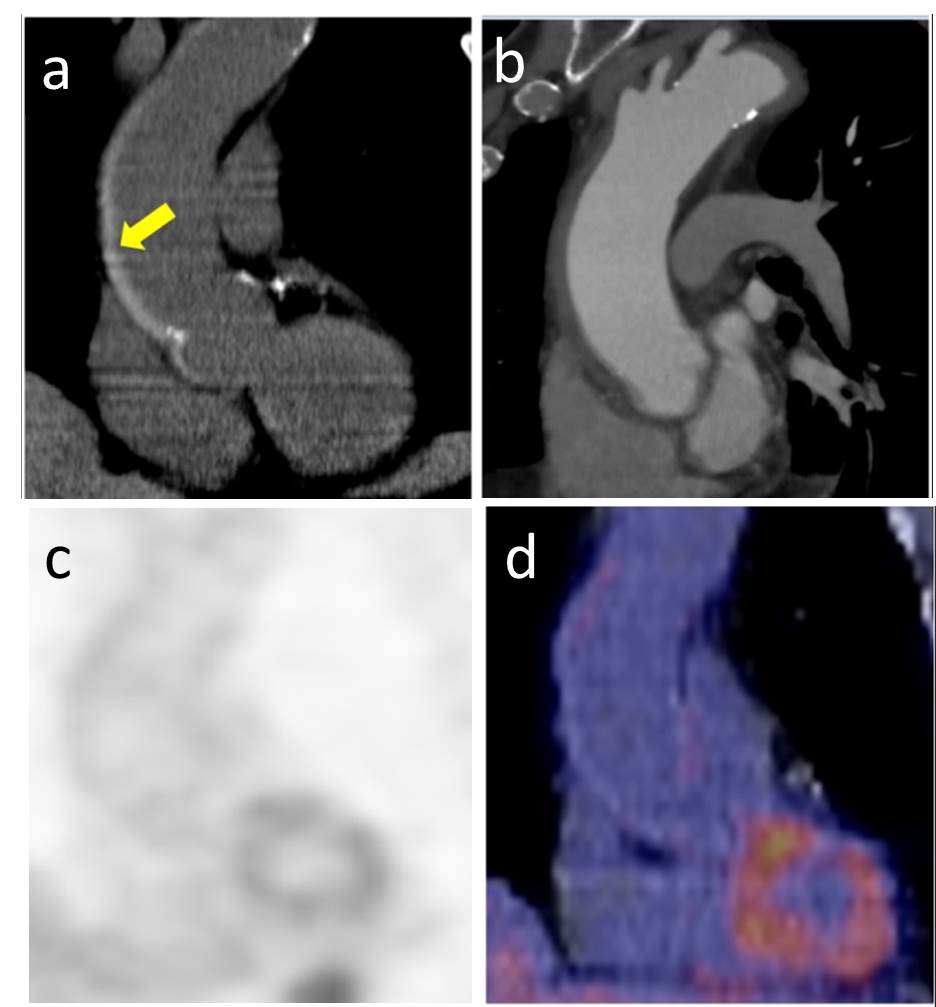
Figure 1: Unenhanced CT of the ascending aorta showing intramural hematoma with high-attenuation crescentric thickening (yellow arrow) on long axial view (a). Contrast-enhanced CT images on long axis view showed a wall-thickened thoracic aorta (b). Attenuated corrected image (c) and fused 18F-FDG-PET CT (d) of the ascending aorta that did not show diffuse 18F-FDG wall uptake.
Imaging Findings:
The magnetic resonance scan of the aorta showed an enlarged and wall-thickened thoracic aorta on cine steady state free precession (SSFP) images. In the T2-weighted images, the aorta wall displayed increased signal compatible with an acute aortic syndrome. Although pre-contrast T1-weighted imaging was not undertaken, post-contrast T1-weighted imaging known as Late gadolinium enhancement (LGE) images for myocardium assessment was applied to the aorta. This demonstrated intimal and adventitial isointesity, with an hypoenhanced band in the aortic wall suggestive of intramural hematoma (Figure 2). The intramural hematoma was confirmed during the surgical repair of the aorta (Video 1).
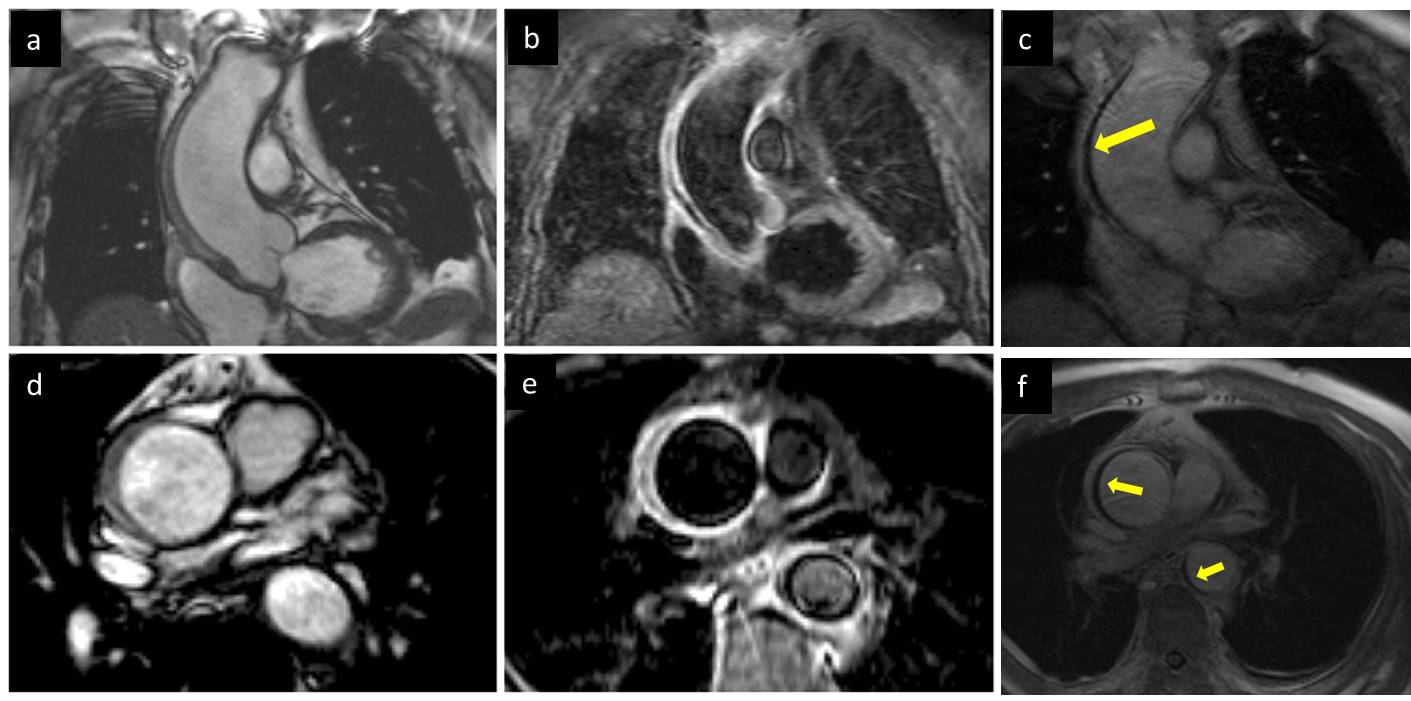
Figure 2: CMR of the ascending aorta showing the thickened aortic wall on cine steady state free precision (SSFP) imaging (a), hyperintense on T2-weighted imaging (b), and late gadolinium enhancement (LGE) imaging (c) showing normal isointense intimal and adventitial, corresponding to aortic wall, and a hypoenhanced band in the aortic wall (yellow arrow), corresponding to intramural hematoma. Corresponding short axis views of the ascending aorta on cine SSFP imaging (d), T2-weighted imaging (e) and LGE imaging (f). Image (f) additionally shows extension of the hematoma to the descending aorta (smaller yellow arrow)
Video 1: Demonstrating intra-operative finding of Intramural Hematoma
Perspective
This case illustrates the ability of myocardial LGE sequences to identify acute aorta intramural hematoma. LGE is a non-invasive established technique for the diagnosis of myocardial fibrosis and necrosis. LGE involves inversion-recovery imaging after intravenous administration of gadolinium contrast and a 5-10 minute delay. With appropriate settings, normal myocardium appears black or nulled, whereas nonviable regions appear bright or hyperenhanced. In addition, magnetic resonance is a well-established technique to identify intraventricular thrombus (3). Thrombus is avascular and has essentially no gadolinium uptake. Therefore, intraventricular thrombus appears black on LGE images (3).
Intramural hematoma is a severe aortic disease consisting of intramural thrombus in the media of the aortic wall in the absence of a false lumen and intimal tear. It is diagnosed in the presence of a circular or crescent-shaped thickening of >5 mm of the aortic wall in the absence of detectable blood flow (1). It is caused by rupture of vasa vasorum of the aortic wall, which is composed histologically of three layers: a thin inner tunica intima lined by the endothelium; a thick tunica media characterized by concentric sheets of elastic and collagen fibers as well as smooth muscle cells; and the outer tunica adventitia containing mainly collagen, vasa vasorum, and lymphatics (2-3). Due to the collagenous and elastic tissue, normal aortic wall appears isointense on LGE images. In our case, late gadolinium enhancement images demonstrate an isointese intimal and adventitial layer with a hypoenhanced band in the middle of aortic wall suggestive of intramural hematoma. Intramural hematoma is displayed on LGE images as a black band in the middle of the aortic wall. This fact can be used to discern thrombus from aortic wall layers. In addition, magnetic resonance characterizes mural edema with T2 “edema weighted” sequences suggesting an acute intramural hematoma. In our case the extent of the edema may surpass the confines of the hematoma, as may be expected due to inflammation around the hematoma. Although not performed here, pre-contrast T1-weighted imaging can also be of value in the these cases. In the case of acute intramural hematoma, the hematoma appears isointense and in subacute hematoma, it appears hyperintense due to the accumulation of iron-rich macrophages. Other medical conditions are associated with presence of a circular thickening of the aortic wall such as aortitis. In patients with aortitis, magnetic resonance may show thickening; wall edema (a marker of active disease) and hyperenhancement on LGE imaging of the arterial wall in patients with aortitis (4-5) but not signs of intramural hematoma on LGE images as it was described in this case.
The majority of cases of acute aortic syndrome can be diagnosed using CT. This case highlights the importance of the unenhanced CT and the utility of cardiac MRI in the setting of any diagnostic uncertainty. Recent ASE/ EACVI guidelines suggest that MRI is extremely accurate in this setting but practicalities may limit the use of this modality to patients requiring serial follow-up.
Conclusion
These findings suggest that LGE images detect aortic intramural hematoma in patients with acute aortic syndrome. Late gadolinium enhancement images can be used to study patients with wall-thickened aorta to identify intramural hematoma and rule out other medical conditions associated with thickening of the aortic wall (e.g. aortitis).
References
- 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 2014;35:2873-2926
- Braverman AC, Thompson RW, Sanchez LA. Diseases of the aorta. In: Bonow RO, Mann DL, Zipes DP, Libby P. Braunwald’s Heart Disease. 9th ed. Philadelphia: Elsevier Saunders; 2012, 1309 – 1337.
- Devereux RB, de Simone G, Arnett DK, Best LG, Boerwinkle E, Howard BV, Kitzman D, Lee ET, Mosley TH Jr., Weder A, Roman MJ. Normal limits in relation to age, body size and gender of two-dimensional echocardiographic aortic root dimensions in persons ≥15 years of age. Am J Cardiol 2012; 110:1189–1194.
- Gornik HL, Creager MA. Aortitis. Circulation 2008; 117:3039 – 3051.529
- Pipitone N, Versari A, Salvarani C. Role of imaging studies in the diagnosis and follow-up of large-vessel vasculitis: an update. Rheumatology (Oxford) 2008; 47: 403 – 408.
- Goldstein SA, Evangelista A, Abbara S, Arai A, Asch FM et al .Multimodality imaging of diseases of the thoracic aorta in adults: from the American Society of Echocardiography and the European Association of Cardiovascular Imaging: endorsed by the Society of Cardiovascular Computed Tomography and Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. 2015 Feb;28(2):119-82
Case Prepared by: Tarique Hussain