



Stephen N. Darty, Anna Lisa Crowley
Duke University Medical Center, Durham, NC, USA
Clinical history
A 43 year old female with a past medical history significant for hypertension and mild rheumatoid arthritis and no known cardiac disease experienced the sudden onset of chest pain, malaise, and pre-syncope at an airport. Paramedics were alerted and she was found to have inferior ST- segment elevations on an ECG (see Figure 1). The patient was immediately taken to the nearest cardiac catheterization laboratory and was found to have no significant coronary artery lesions. Her peak CK-MB was in the 50s ng/mL and her peak Troponin was 15 ng/mL. A transthoracic echocardiogram demonstrated an inferior wall motion abnormality and a left ventricular ejection fraction of 35-45% (see Figures 2-6). Her symptoms and inferior ST segment elevations subsequently resolved. She was diagnosed with coronary vasospasm and treated with diltiazem, carvedilol, aspirin, clopidogrel, nitroglycerin, simvastatin, and lisinopril. After discharge, she participated in cardiac rehabilitation but reported low energy and fluid retention that was managed with low-dose diuretics.
She did not have recurrent chest pain until seven months after the initial discharge when she had another episode of chest pain with pre-syncope. She reported to another outside hospital. Her ECG demonstrated inferior ST-segment elevation with Q-waves. She emergently underwent coronary angiography and, again, had no significant coronary artery disease. Her peak CKMB was noted to be in the 60s ng/mL. She was again presumed to have coronary vasospasm and her diltiazem dose was increased. Since her 2nd hospital discharge, the patient reported no further chest pain, but endorsed low energy and edema that resolved with diuretics. She did, however, develop significant anxiety about her condition so presented to our institution for a second opinion.
Figure 1. Inferior ST segment elevations
Figure 2. Parasternal long axis view
Figure 3. En face view of aortic valve
Figure 4. Short axis view
Figure 5. Non-zoomed para sternal long axis view
Figure 6. Non-zoomed parasternal long axis view with color
A cardiac MRI was ordered to evaluate for scar burden and etiology of heart failure. Initial functional images were performed on a 3.0 T MRI system using steady state free precession (SSFP) cine images with a 6mm slice thickness and temporal resolution <40msec (Figures 7-12). These images demonstrated an inferior wall motion abnormality with a quantitative LVEF of 40%.
Figure 7. Long axis view & Figure 8. Four chamber view
Figure 9. Two chamber view & Figure 10. Basal short axis view
Figure 11. Mid short axis view & Figure 12. Apical short axis view
Upon completion of non-contrast SSFP functional imaging gadolinium contrast was administered and free breathing single-shot SSFP delayed enhancement images were acquired with an inversion time set high (875 msec) for intracardiac thrombus detection (per routine departmental protocol) in the short axis (Fig 13) and 2 chamber view (Fig 14). These sequences demonstrated a hypointense mass on the aortic valve.
Figure 13. Short axis high TI single shots & Figure 14. Two chamber high TI single shots
Post contrast, the aortic valve was again imaged with SSFP sequences. Surprisingly the lesion noted on the SSFP DE-CMR images were not demonstrated on the SSFP cines (Figures 15-16).
Figure 15. SSFP LVOT cine & Figure 16. SSFP en face aortic valve cine
Free breathing single-shot null inversion time images were then performed (Fig 17-18) for detection of myocardial infarction and fibrosis. In addition to the transmural myocardial infarction (which corresponds to ECG and functional imaging) an etched lesion now appears on the aortic valve in the same region noted on high TI images acquired earlier (Fig 13-14).
Figure 17. Short axis high TI single shots & Figure 16. Two chamber high TI single shots
The cardiac MRI technologist localized the lesion from the single shot techniques with a SSFP functional image (Fig 19) that is slightly off axis for the left ventricle, but purposefully dissects the lesion. This still does not demonstrate any abnormality.
Figure 19. Off axis three chamber SSFP cine through the lesion
Fast Gradient Echo imaging (FGRE) imaging techniques were then used. FGRE techniques generally are lower in signal to noise and temporal and spatial resolution, but offer a T1 weighted cine image rather than the T2/T1 weighted cine images produced by SSFP imaging. FGRE imaging nicely demonstrates a mass on the right coronary cusp of the aortic valve at the ostium of the right coronary artery (Fig 20-21). This lesion was presumed to intermittently embolize and/or occlude the right coronary artery causing the patient’s inferior myocardial infarction.
Figure 20. Off axis three chamber FGRE cine
Figure 21. En face aortic valve FGRE cine
A differential diagnosis for the mass was thrombus, vegetation from infective endocarditis, or non-bacterial Libman-Sacks endocarditis. A white blood cell count and ESR were normal and blood cultures were negative. The diagnosis of endocarditis was excluded (both bacterial and non-bacterial). The patient was referred for surgical resection of the mass due to recurrent embolization despite anticoagulation.
Intraoperative TEE demonstrates the mass on the right coronary cusp of the aortic valve (fig 22in long axis and fig 23 in short axis) which was subsequently resected with preservation of the native aortic valve.
Figure 22. Intraoperative TEE
Figure 23. Intraoperative TEE en face aortic valve cine
Surgical pathology was consistent with fibroelastoma because of site of origin and the gross morphology of the primary mass with rare peripheral suggestion of papillary morphology. The histology was somewhat atypical because of the lack of numerous central fibrovascular cores with elastin and the prominent myxoid component with strong CD34 staining. (see Fig 24)
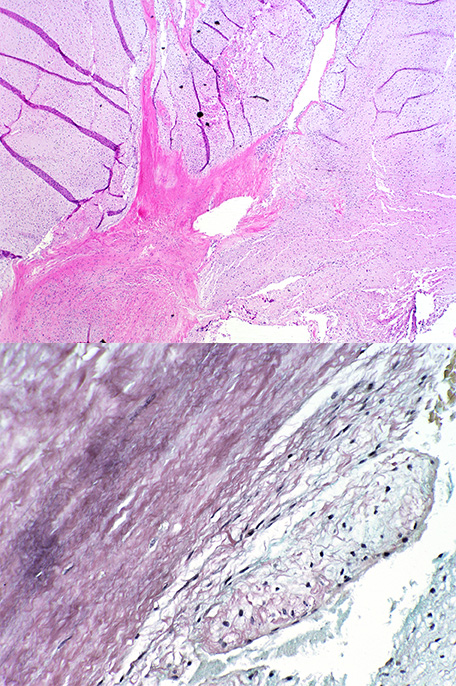
Figure 24. Surgical pathology slides from atypical papillary fibroelastoma.
Perspective
Primary tumors of the heart are rare and in most cases benign. While the nature of the tumor may be benign, it’s effects on the heart can cause symptoms of right and left sided heart failure as well as myocardial infarction [1]. Papillary fibroelastomas are the third most common benign primary cardiac tumor and are often found by echocardiography alone[2]. Cardiac MRI can provide additional insight and tissue characterization in detection and characterization of primary cardiac tumors. Utilizing additional pulse sequences that offer different T1 and T2 tissue characteristics is important in not only helping to understand the composition of masses, but also in identification. In this case T1 weighted delayed enhancement and T1 weighted FLASH sequences were vital to discovering this mass which was not seen on SSFP T2/T1 weighted pulse sequences. MRI is not limited by poor acoustic windows and can also be helpful in patients when the diagnosis is unclear.
Click here to see complete case in CloudCMR.
References

