



Case from: Bansmann PM, Stamm I, Al Sayari S
Institution: KardioMR Cologne/Bonn, Krankenhaus Porz am Rhein, Cologne, Germany.
Clinical history: A 43 year old male presented with history of dyspnea on exertion and family history of sudden cardiac death. Initial workup with an echocardiogram demonstrated normal left ventricular function and no wall motion abnormalities. The patient was referred for evaluation of possible coronary artery disease for which he underwent an cardiac CTA.
320-Row-Volume-CT: Normal coronary arteries without any atheromatous or atherosclerotic changes. No intraluminal stenosis was seen. The right ventricle and right atrium appeared generous without any detectable septal defects. The CTA also showed limited coverage of the left atrium in the cranial aspect (head-feet: 16 cm) without a clear anatomical drainage of the left pulmonary vein (LUPV (Figure 1). Thus an aberrant LUPV was suspected. A CMR and MR-Angiography was obtained for further followup.

Figure 1
CMR: The right atrium and ventricle were mildly dilated with normal right ventricular systolic function. The left ventricular chamber size was normal with normal systolic function (Movie 1). In navigator triggered HASTE-sequence a tubular structure was seen to the left of the aortic arch (Movie 2, Figure 2).

Movie 1

Movie 2

Figure 2
MR-Angiography: Normal anatomy and diameter of the pulmonary trunk. Normal diameters and anatomy of the RUPV, RLPV and LLPV. The MR-Angiography clearly reveals the aberrant LUPV with drainage into the persistent left SVC (pLSVC) which drains into brachiocephalic vein without additional anatomical abnormalities (Figure 3).
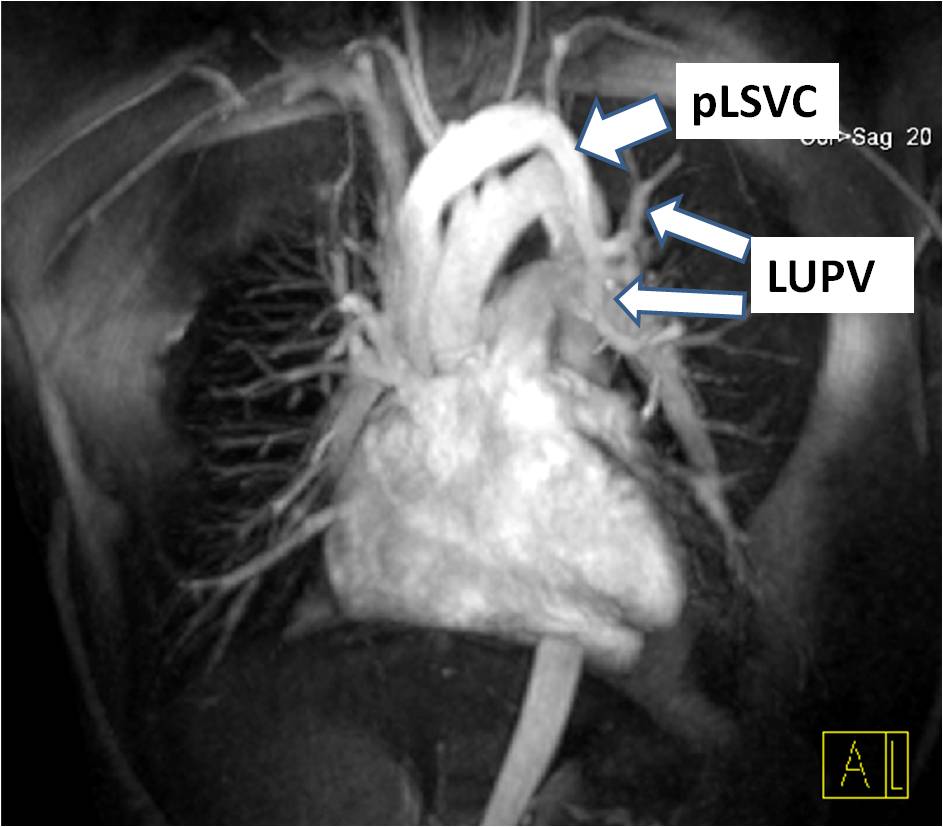
Figure 3
Flow measurements: Comparing flow in the pulmonary trunk and ascending Aorta a difference of 20 cc in antegrade flow volume is measured. Total stroke volume of the left ventricle is 98cc. The QP:QS calculated was 1.2:1.
Conclusion: Despite the cardiac volume acquisition by CTA the vascular anomalies cannot be competely outlined due to the restricted field of view prescribed to limit radiation exposure. CMR has the unique advantage of a wider field of view acquisition as there is no radiation involved. Additionally, CMR provides important hemodynamic information about the right heart size, function and shunt quantitation.
Author’s Comment: The edited conclusion doesn’t reflect our interpretation of the significance of both cardiac volume CT and MRI. Limitation of volumetric coverage in CT isn’t done to reduce radiation exposure. It’s an intrinsic limitation due to detector width. As stated in our conclusion both modalities are a valuable contribution to finding the correct diagnosis and are complementary to each other.
Case Handling Editor: Vikas K. Rathi