



Case from: Majid Asawaeer & Vincent Sorrell
Institute: Division of Cardiology, Department of Internal Medicine, University of Arizona, Tucson, Arizona, USA
Clinical history: A 65 year old female patient with severe, symptomatic mitral regurgitation underwent mitral valve repair for posterior mitral valve leaflet restriction (type IIIb). Pre-operative assessment of the coronary tree was reported as normal. At surgery, the left atrial wall appeared abnormal and a left atrial biopsy was performed. Surprisingly, histological examination of this biopsy showed chronic, non-caseating granulomatous changes suggestive of sarcoidosis.
CMR was subsequently performed to assess for possible myocardial involvement from cardiac sarcoidosis.
Movie 1 Steady state free precession cine, 2-chamber view focal basal

Movie 2 Steady state free precession cine, 3-chamber view, showing a infero-lateral wall motion abnormality
Movie 3 Steady state free precession cine, short axis image of the basal left ventricle.
A focal wall motion abnormality is well demonstarted in the infero-lateral region (4 o’clock).
CMR Findings: the CMR study was acquired post-operatively, with significant susceptibility artefacts following the mitral intervention and annuloplasty ring. SSPF cine images revealed a normal global left ventricular ejection fraction (LVEF: 64%;) despite a limited akinetic region in the basal infero-lateral segment (Movie 2 & 3). The global RV ejection fraction was normal. The left atrium was dilated.
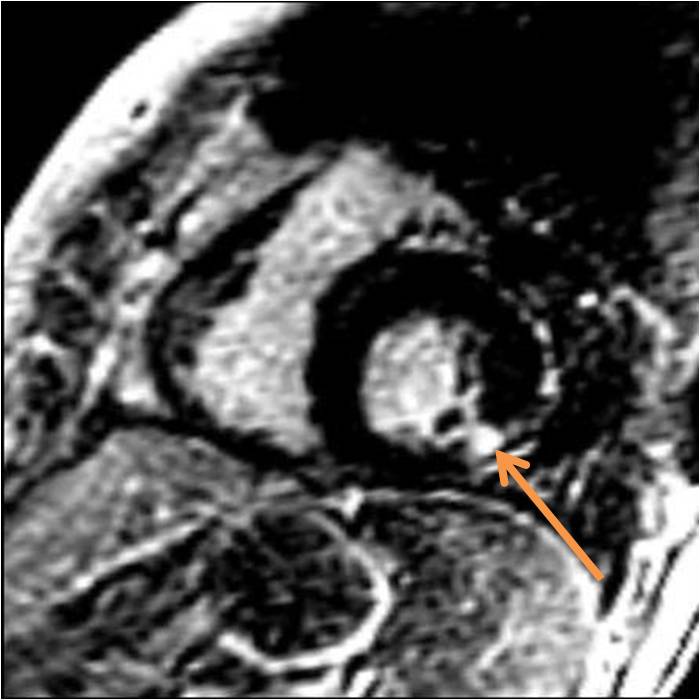
Figure 1 Delayed enhancement sequence at the same orientation and location as Movie 3. Note the very focal bright region of enhancement (arrow) in the subepicardial (non-CAD pattern) region
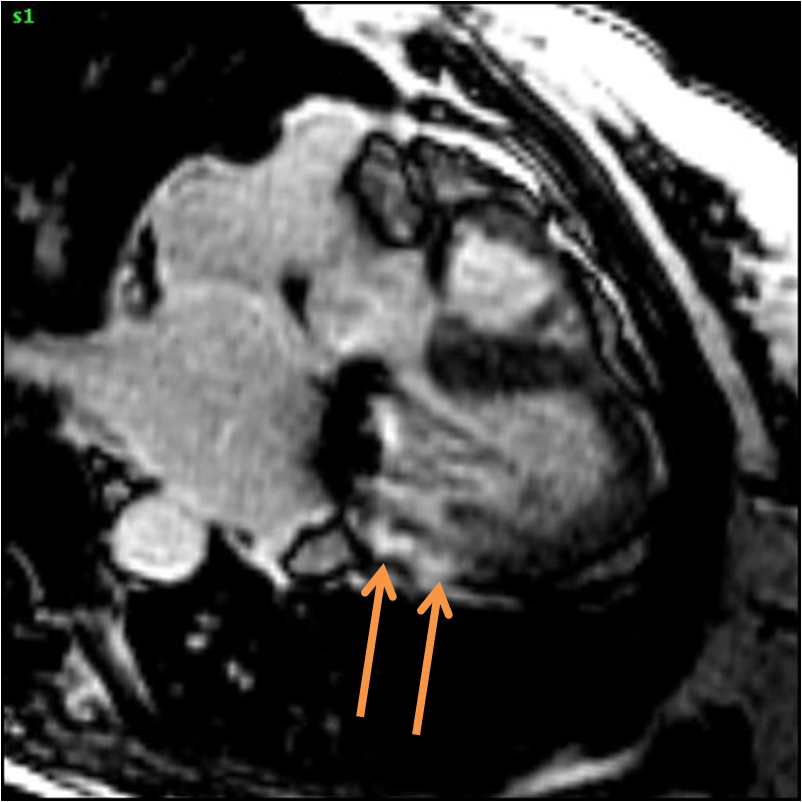
Figure 2 Delayed enhancement sequence at the same orientation and location as Movie 2 (3-chamber view). Note the very focal bright region of enhancement (arrows) in the basal infero-lateral wall matching the wall motion abnormality
Delayed enhancement images after gadolinium confirmed the presence of a focal fibrosis matching the wall motion abnormality previously described (Figures 1 & 2). There also appeared to be fibrosis involving a large segment of the thickened atrial wall (Figure 3).
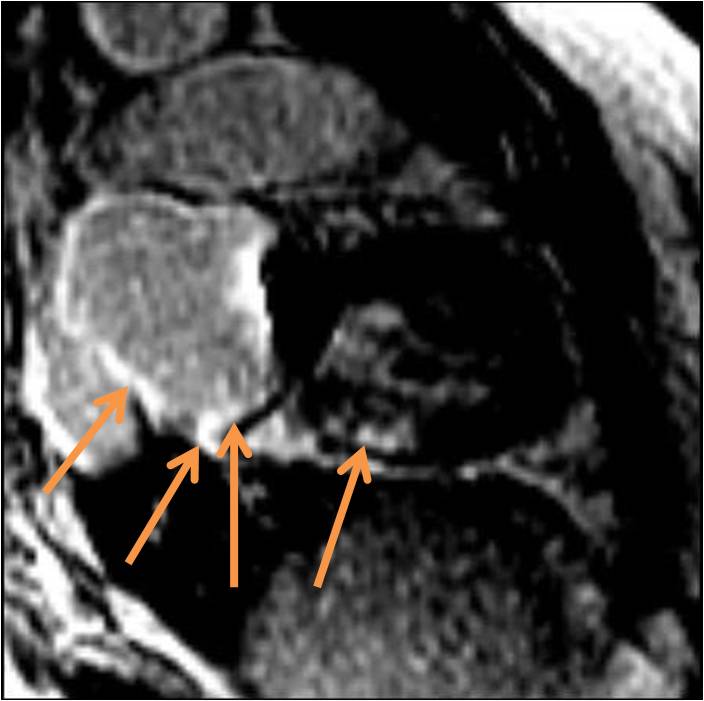
Figure 3 Delayed enhancement sequence in an axial, long axis orientation showing the focal left ventricle scar (arrow) Additionally, the left atrial wall is markedly enhanced (arrows).
Perspective:
Cardiac sarcoidosis is an underdiagnosed disease as it may be asymptomatic despite pulmonary involvement. Furthermore, it may be the presenting feature of sarcoidosis – as in our case – with a cited prevalence of 20% to 25%.1
Cardiac involvement may be present in the absence of any abnormality on standard cardiac testing and CMR is becoming the noninvasive diagnostic imaging technique of choice for evaluation and diagnosis of suspected cardiac sarcoidosis. 2
Mitral regurgitation (MR) may occur in the setting of cardiac sarcoidosis due to associated systolic dysfunction and left ventricular dilation or due to papillary muscle involvement by sarcoid granulomas 3. Focal involvement of the infero-lateral wall associated with left artial involvement likely also contributes to the MR.
Cardiac sarcoidosis should be considered in patients presenting with unexplained mitral regurgitation. Our review of the literature suggests this is at least the 4th reported case of cardiac sarcoidosis presenting as mitral regurgitation.
CMR could be considered in all non-ischemic mitral regurgitation where the etiology of mitral regurgitation is not clear. In this case, CMR added information over and above the surgical biopsy of the left atrium
References:
- F. Tavora, N. Cresswell and L. Li: Comparison of necropsy findings in patients with sarcoidosis dying suddenly from cardiac sarcoidosis versus dying suddenly from other causes. Am J Cardiol 2009; 104(4):571-577.
- E. Tadamura, M. Yamamuro and S. Kubo: Effectiveness of delayed enhanced MRI for identification of cardiac sarcoidosis: comparison with radionuclide imaging. AJR Am J Roentgenol 2005;185(1):110-115.
- Sato Y; Matsumoto N; Kunimasa T; Imai S; Matsuo S; Nakano Y; Yoda S; Kunimoto S; Saito S; Hirayama A: Multiple involvements of cardiac sarcoidosis in both left and right ventricles and papillary muscles detected by delayed-enhanced magnetic resonance imaging. Int J Cardiol. 2008;130(2):288-90.
- F. von Knobelsdorff-Brenkenhoff, J. Schulz-Menger: Cardiac Sarcoidosis – CMR assessment in the acute phase and at follow up. Case of the Week Number 10-11.
COTW handling editor: Monica Deac

