



Case from: G Cooper, R Shifrin & J Peterson.
Institute: University of Florida Cardiac Imaging Group, Gainesville, Florida, USA.
Clinical history: A 64 year old female with acute myocardial infarction 20 years earlier and CABG 10 years previously, was admitted with 2 episodes of syncope. Physical examination was positive for a well healed median sternotomy and an S4. Cardiac markers were twice negative.
EKG shows normal sinus rhythm at rate of 62 bpm, loss of R wave anteriorly and T wave abnormalities in DI, aVL and the anterior precordial leads (Figure 1).
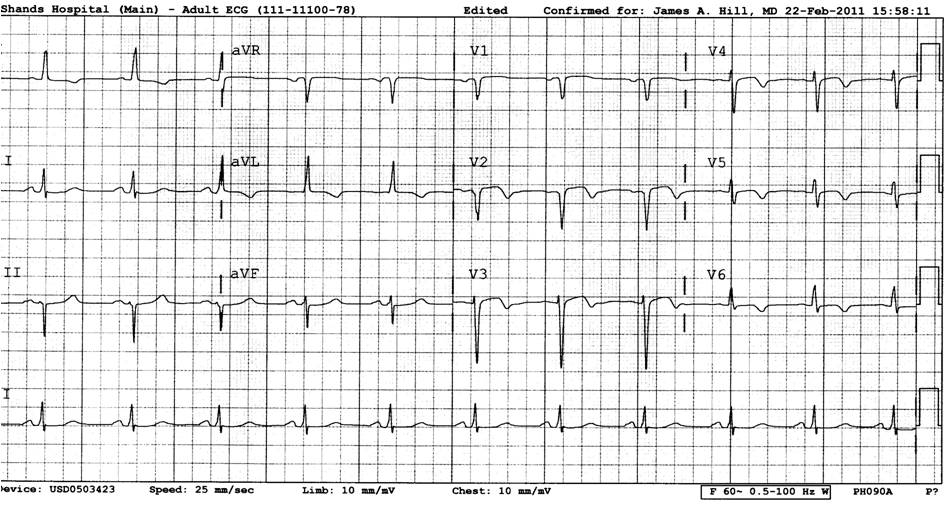
Figure 1
SPECT Regadenoson stress perfusion study (not shown) demonstrated a large, severe, fixed, anterior perfusion defect.
Transthoracic echocardiography showed a dysfunctional LVEF of ~40%, with anteroseptal and apical hypokinesis.
CMR was ordered in consideration of bi-ventricular pacing therapy.
CMR Findings: except as noted, images were obtained prior to the injection of Gadolinium.
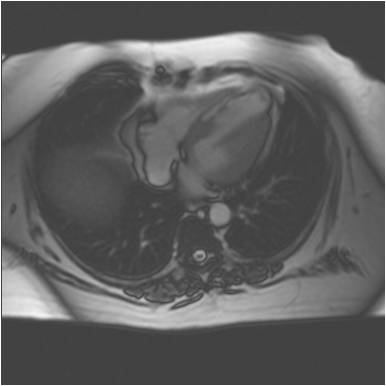
Figure 2 – Axial Localiser showing apical thinning with an area of increased signal intensity from the ventricular septum
The first transaxial localiser images already show apical thinning of the LV with an area of increased signal intensity in the interventricular septum (Figure 2).

Movie 1 & Movie 2
4 & 2 chamber steady-state free precession (SSFP) cines (Movies 1 & 2) demonstrate an area of high signal intensity in the septum (previously seen on the axial localiser – Figure 2) with anterior and apical wall thinning and dyskinesis.
Movie 3
On the short axis SSFP cines (Movie 3), the anterior and anteroseptal dyskinesis and thinning is well observed. The area of increased signal in the interventricular septum is noted once again.


Movie 4 & Movie 5

Movie 6
Resting Gadolinium perfusion images were obtained in 3 short axis slices (Movies 4 [base], 5 [mid-cavity level] and 6 [apex]). The septal area with increased signal intensity was once again noted before the injection of Gadolinium. There is a thin rim of hypoperfused subendocardial myocardium seen on all three stress slices.
A standard set of multi-plane late gadolinium-enhanced (LGE) images was obtained (Movie 7 [short axis stack] & Movie 8 [4-chamber view]). It was evident that the preexisting septal area of increased signal intensity would make assessment of concomitant LGE in the same area problematic.


Movie 7, Movie 8, Movie 9, and Movie 10
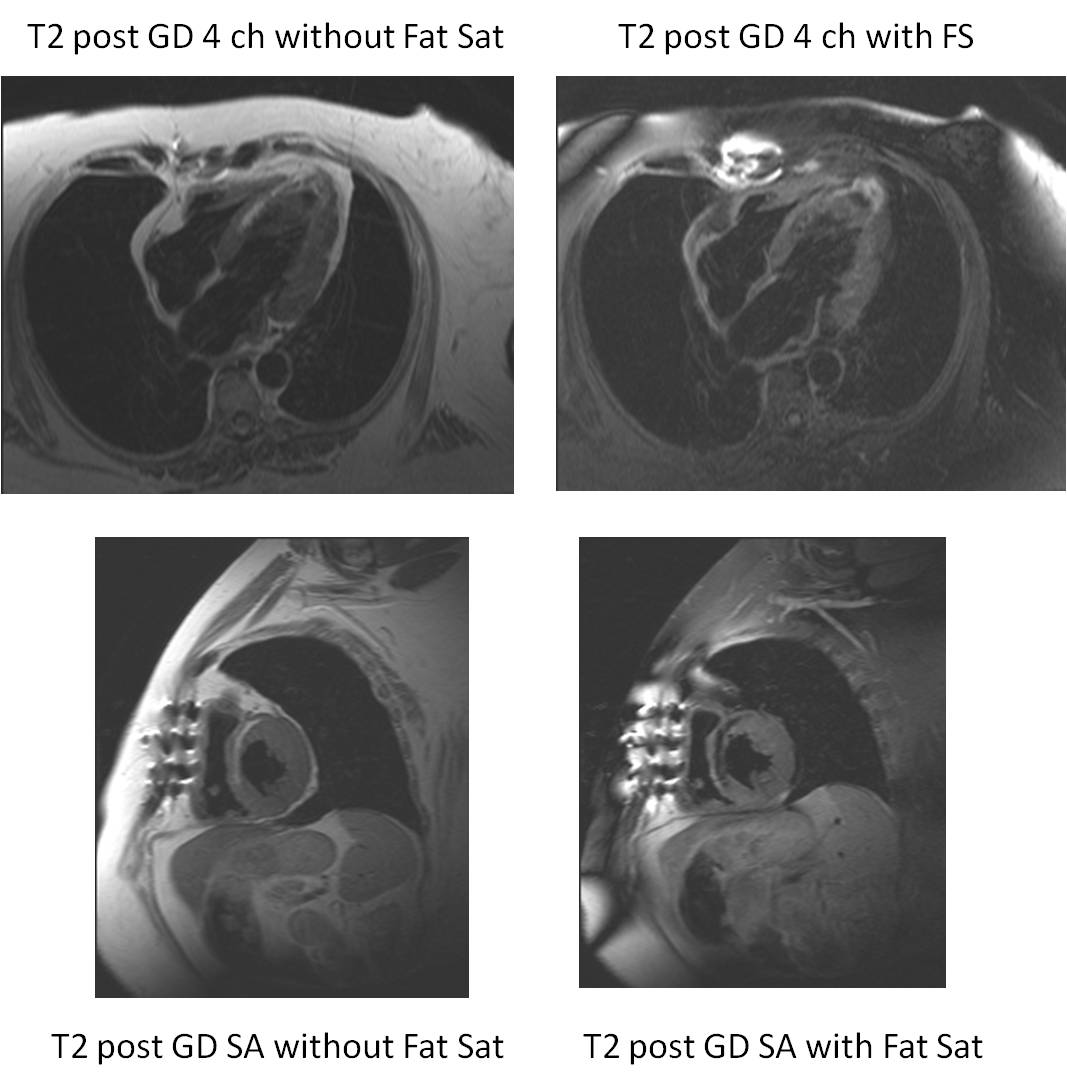
Figure 3
Finally, T2-weighted post Gadolinium images in the the 4 chamber view (Figure 3 upper panel) and in the short-axis orientation (Figure 3 lower panel) without fat saturation (Figure 3 left panel) and with fat saturation (Figure 3 right panel)were obtained. This demonstrated that the area of increased signal intensity in the interventricular septum is fat, localised in the area of the previous myocardial infarction.
Perspective: Fatty metamorphosis is a complication of acute myocardial infarction. There exist sporadic reports(1,2) of fatty change following myocardial infarction. In a series of 25 post myocardial infarction patients, 18 of which had CMR-demonstrable fatty changes, there was a high prevalence of fatty metamorphosis in patients with large infarct volume, decreased LV EF, increased LV ESV index, and increased LV Mass(3).
Autopsy studies (4,5) have demonstrated a high incidence of fatty change following myocardial infarction. Fatty metamorphosis such as demonstrated here may be more common than previously appreciated.
It may be difficult to identify areas of late gadolinium enhancement in the presence of fat, since both have high signal intensity. The judicious use of multi-plane Look-Locker series at various TIs may demonstrate early nulling in the infarct area. T1 pre Gadolinium or T2 pre or post Gadolinium images without and with fat saturation can confirm the diagnosis of fatty metamorphosis. The fatty metamorphosis was largely in the mesocardium. The dark line encircling the fatty area is likely to represent a chemical shift artifact.
References:
- J Estornell, R Jimenez, F Ridocci: In Vivo Demonstration of Lipomatous Metaplasia in Left Ventricular Scar Following Myocardial Infarction. Eur Heart J 2006, 27(15): 1766.
- Sung Soo Ahn1, Young-Jin Kim, Jin Hur, Hye-Jeong Lee, Tae Hoon Kim, Kyu Ok Choe and Byoung Wook Choi : CT Detection of Subendocardial Fat in Myocardial Infarction. AJR 2009; 192:532-537.
- JW Goldfarb, M Roth, J Han: Myocardial Fat Deposition after Myocardial Infarction. Radiology 2009;253(1):65-73.
- Baroldi G, Silver MD, De Maria R, Parodi O, Pellegrini A: Lipomatous Metaplasia in Left Ventricular Scar. Can J Cardiol 1997;13:65-71.
- L Sul, JE Siegel, MC Fishbein: Adipose Tissue in Myocardial Infarction. Cardiovasc Pathol 2004;13:98-102.
Submit your case here
COTW handling editor: Monica Deac
Have your say: What do you think? Latest posts on this topic from the forum

