



Case from:Dr Robert Huggett
Institute: Russells Hall Hospital, Dudley, UK.
Clinical history: A 61 year old gentleman presented with worsening breathlessness for 2 years. He had a past history of COPD and idiopathic pericardial constriction which had been treated many years earlier by pericardial stripping through a median sternotomy. His JVP was raised and so he had a transthoracic echocardiogram (Movie 1). This showed a posterior echo-free mass distorting the cardiac structures. A subsequent CT thorax (Fig 1) showed this was a calcified collection and he was then referred for a CMR study to evaluate the mass and its effects.

Movie 1: parasternal long-axis echo view showing a posterior round mass (low left in the image), compressing and distorting the LV (middle in the image)

Figure 1
CMR Findings:
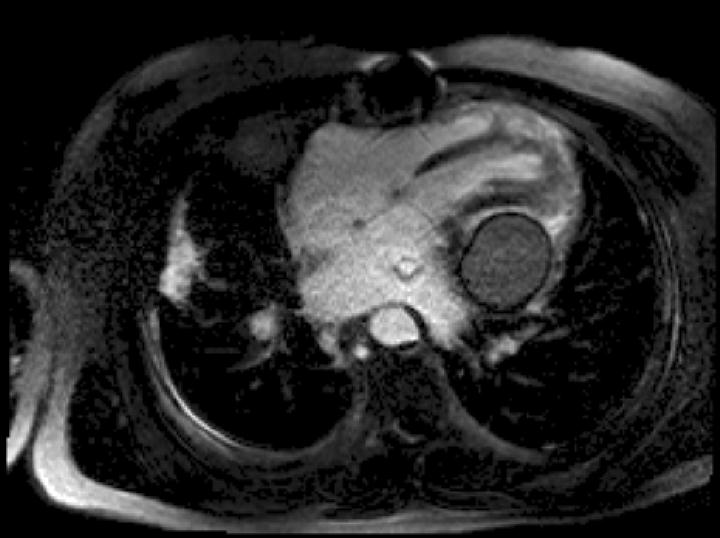
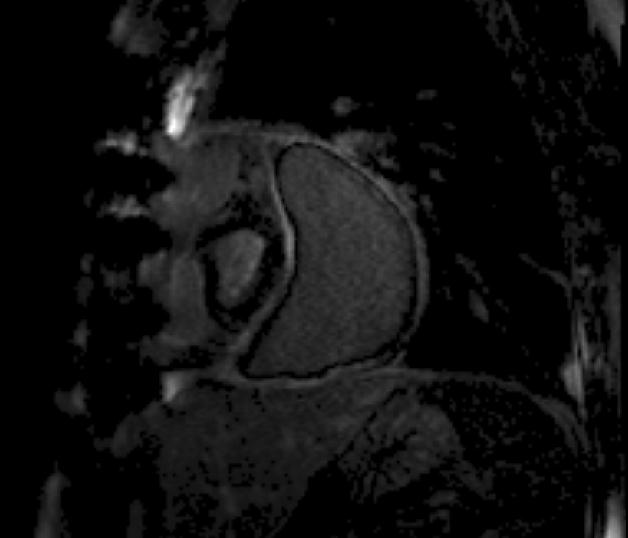
Cine CMR : There is compression of the left ventricle adjacent to the left AV groove by a large posterior pericardial collection. There is residual pericardial thickening (6mm) around the collection with signal drop out due to likely calcification. There is a diastolic IV septal bounce noted and moderate inspiratory diastolic IV septal flattening (Movie 2 and 3).

Movie 2 & Movie 3
Real time imaging: In a short axis view shows near invagination of the interventricular septum on inspiration, normalising on expiration. This characterises ventricular:ventricular interaction, typical of constrictive physiology (Movie 4).

The pericardial collection has typical low to intermediate SI on T1 weighted and high signal on T2 weighted Imaging and SSFP Imaging. There was superimposed fat noted in the left AV groove. There was no early or late gadolinium imaging enhancement (Figure 2).

T1-weighted TSE

T2-weighted TSE
Inversion-Recovery Early Gadolinium Enhancement
Inversion-Recovery Late Gadolinium Enhancement
T2-weighted TSE with fat suppression
Conclusion: The cause of this gentleman’s breathlessness was a localised pericardial collection causing residual constriction of the ventricles with haemodynamic compromise. The patient has been referred for a further cardiothoracic surgical opinion.
Perspective:
This case demonstrates that after an apparent sub-total pericardiectomy, there can be late pericardial problems. This CMR study demonstrated the tissue characterisation and haemodynamic effects of the patient’s problem. Furthermore scanning at 3T may have had an advantage of visualising the pericardium as there is more chemical shift effect.
Pericardial diseases that produce inflammation can cause the pericardium to adhere to the epicardial surface, inducing chronic pericardial constriction. Because of calcification and dense adhesions, pericardial resection can be a technical challenge. The lack of a surgical plane can make this a very difficult operation and defining the best surgical approach for pericardiectomy has been a problem1. The pericardium should be excised from phrenic nerve to phrenic nerve, and also posteriorly, particularly around the entrance of the vena cavae and pulmonary veins to the pericardium2. Late complications after pericardiectomy are thought to be related to the amount of remaining pericardium, the aetiology and severity of the disease.1,2 Operative mortality has been reported as high as 10% to 20%1 and varies based on severity of heart failure, elevation of right atrial pressure, and comorbidities1,2. Although surgery improves symptoms in the vast majority of patients, long-term results are disappointing especially in older patients1,3,4.
References:
1. Ling LH, Oh JK, Schaff HV, Danielson GK, Mahoney DW, Seward JB, Tajik AJ. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy.Circulation 1999; 100:1380-86.
2. Piehler JM, Pluth JR, Schaff HV, Danielson GK, Orszulak TA, Puga FJ. Surgical management of effusive pericardial disease. Influence of extent of pericardial resection on clinical course. J Thorac Cardiovasc Surg 1985;90: 506–16
3. Young PM, Glockner JF, Williamson EE, Morris MF, Araoz PA, Julsrud PR, Schaff HV, Edwards WD, Oh JK, Breen JF. MR imaging findings in 76 consecutive surgically proven cases of pericardial disease with CT and pathologic correlation. Int J Cardiovasc Imaging. 2012; 28:1099-109.
4. Verhaert D, Gabriel RS, Johnston D, Lytle BW, Desai MY, Klein AL. The role of multimodality imaging
in the management of pericardial disease. Circ CardiovascImaging. 2010;3:333-43.
Members only:
How to image the pericardium (Christopher M. Kramer)
COTW handling editor: Giovanni Quarta
Have your say: What do you think? Latest posts on this topic from the forum