



Case from: Mark Michael, DO1; Tracey Hoke, MD1; Kimberly Dunsmore, MD2; Andrew Hoyer, MD1.
Institute: 1University of Virginia, Department of Pediatrics, Division of Pediatric Cardiology, Charlottesville, VA, USA. 2University of Virginia, Department of Pediatrics, Division of Hematology/Oncology, Charlottesville, VA, USA.
Clinical history: A 6 year old girl was referred to pediatric cardiology for evaluation of a heart murmur. Within the past month prior to evaluation, she had been diagnosed with Bell’s palsy. She was asymptomatic from a cardiac standpoint without any chest pain, dyspnea, palpitations or syncope. Physical exam was significant for a harsh early systolic murmur and left lower facial paralysis. An echocardiogram was obtained (Phillips IE33) with relevant images shown below.
Echo 1: Parasternal long axis demonstrates mass along the right ventricular outflow tract as well as echobright tissues within the atrioventricular groove. There is a pericardial effusion.
The patient was admitted with a preliminary diagnosis of lymphoma based on echocardiographic findings. Cardiac MRI (Siemens 1.5 Tesla Avanto) with anesthesia was obtained in addition to other imaging to aid in the diagnosis.
CMR Findings:
MRI 1: Four chamber steady state free precession cine image obtained after administration of gadolinium contrast demonstrates normal ventricular function. Dark signal of different intensity than the myocardium were noted within the atrioventricular groove and base of the left ventricle. These areas correlate with findings seen on echocardiogram.

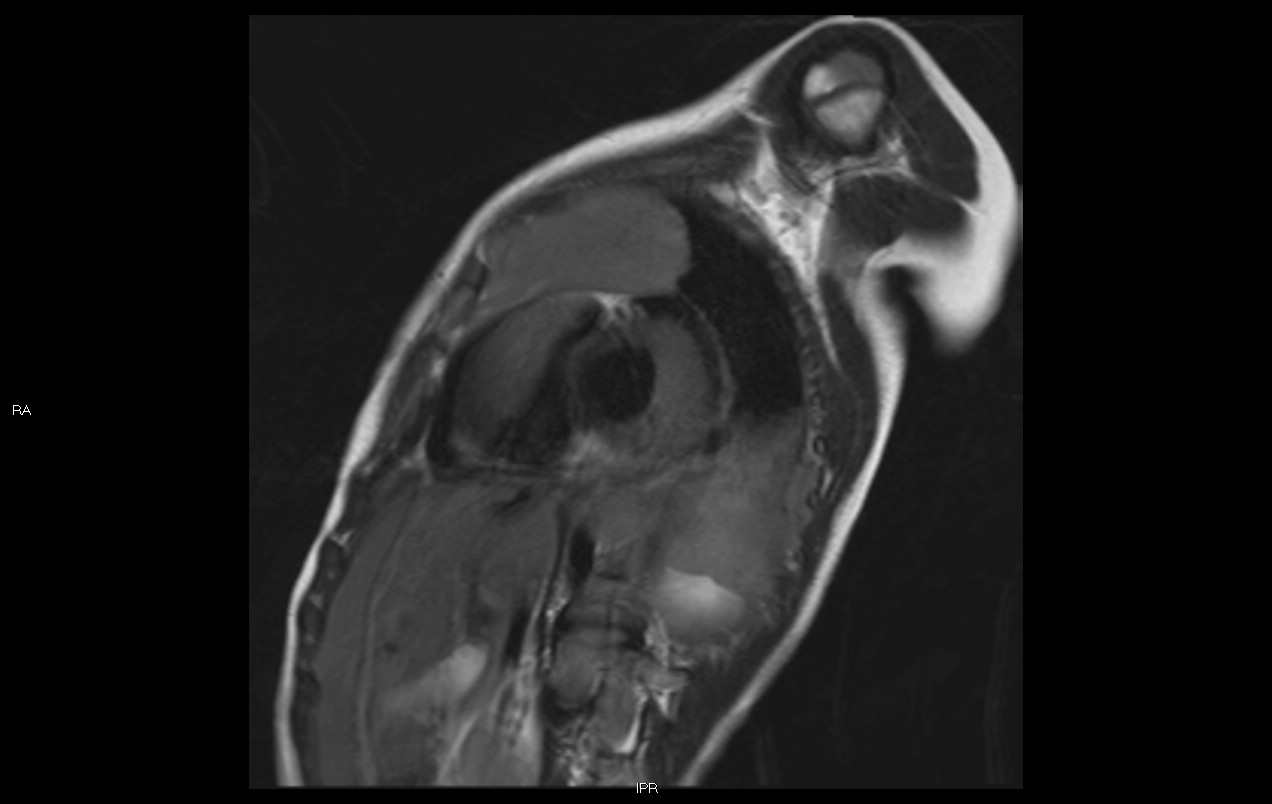
MRI 2: Sagittal steady state free precession cine image obtained after contrast demonstrates involvement of mass along right ventricular free wall and significant impingement upon the right ventricular outflow tract (RVOT). There is flow disturbance through the RVOT which was the likely source of the murmur noted on physical exam.
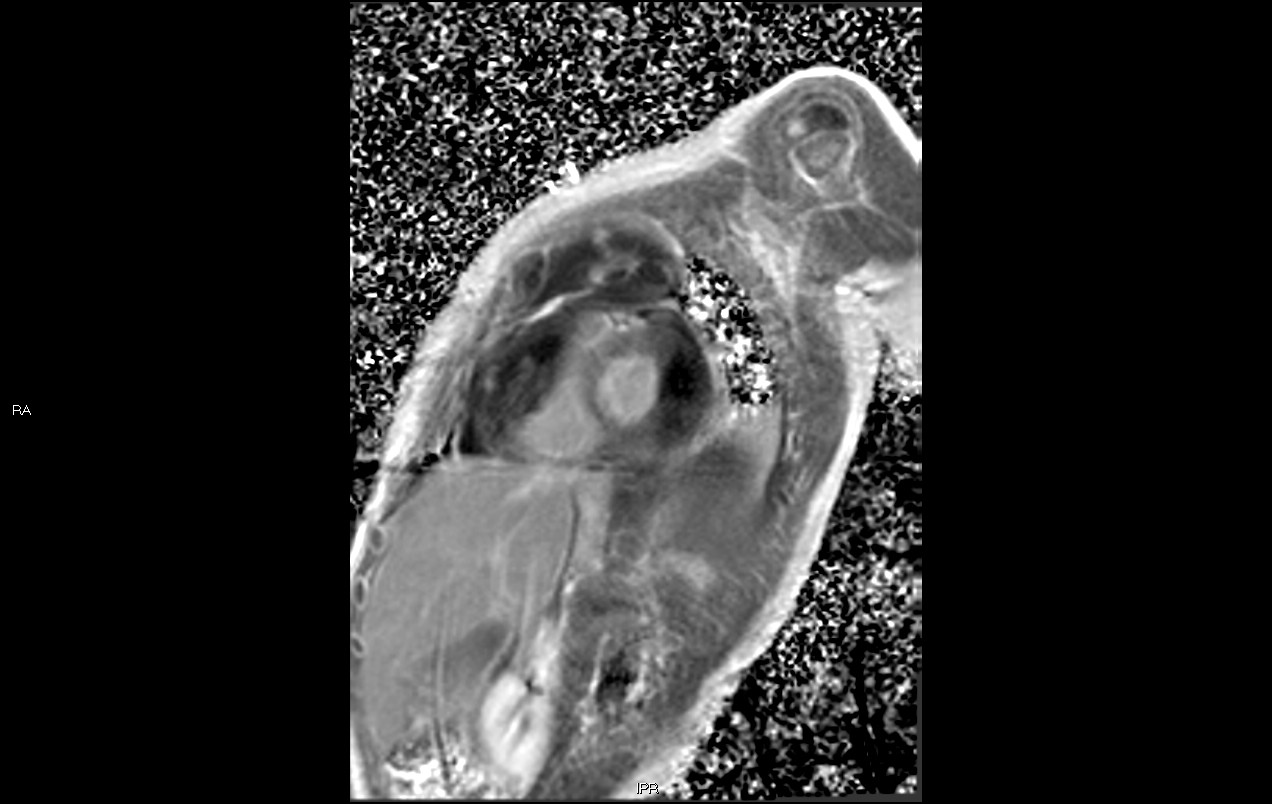
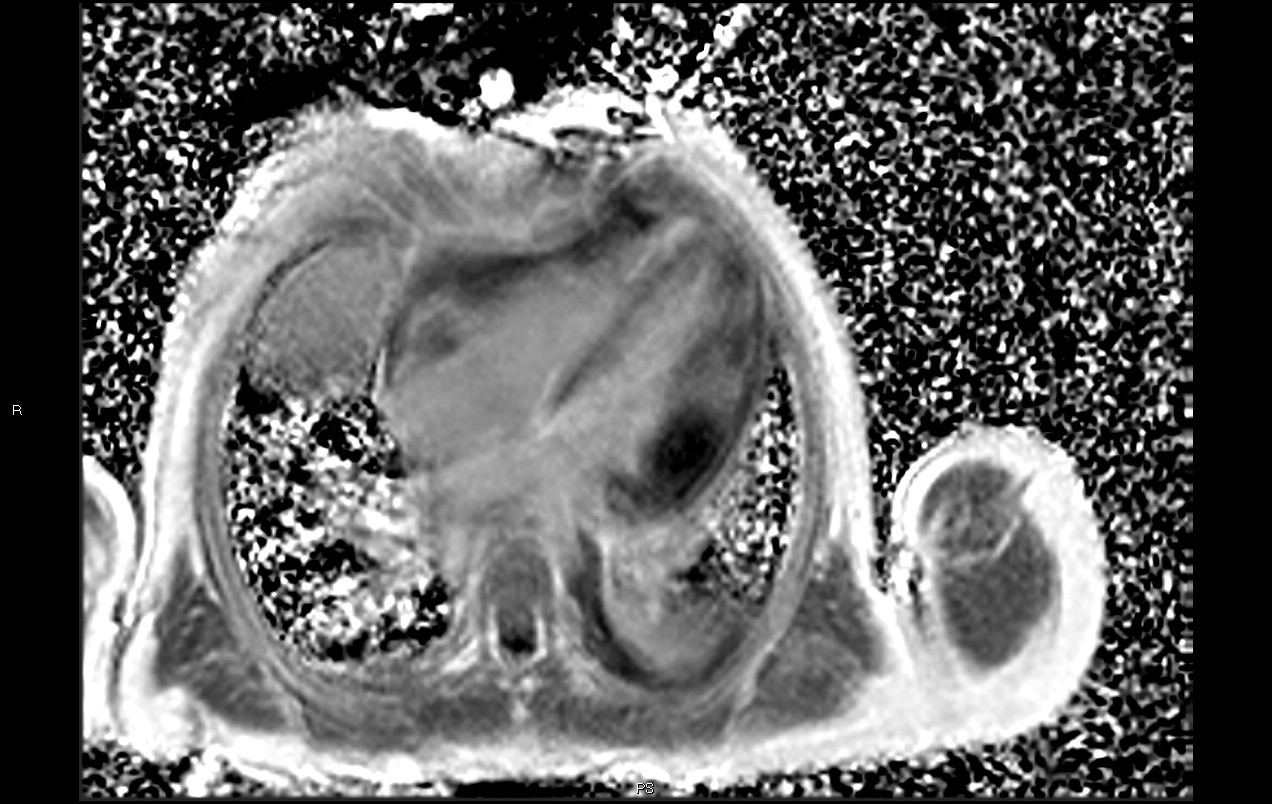
MRI 3 & 4: Perfusion images in the four chamber and short axis planes do not demonstrate enhancement thus excluding a vascularized structure such as a hemangioma.
MRI 5: Spin echo T2 weighted image in short axis plane demonstrates large anterior mediastinal mass. There is no edema of the mass or myocardium. There is a pericardial effusion.
MRI 6: Phase sensitive inversion recovery with late gadolinium enhancement in the short axis plane does not enhance and therefore not indicative of fibrosis.
MRI 1 & 7: Phase sensitive inversion recovery with late gadolinium enhancement in the four chamber plane does not enhance and therefore not indicative of fibrosis. MRI 1 is a 4 chamber SSFP image provided for comparison to the phase sensitive inversion recovery with late gadolinium enhancement.
Conclusion: She ultimately underwent surgical biopsy of the anterior mediastinal mass. Histopathologic and immunohistochemistry analysis were consistent with a diagnosis of T cell lymphoblastic lymphoma. Steroid therapy was initiated, and she subsequently underwent chemotherapy with resolution of the cardiac mass and the cardiac murmur after 4 weeks of therapy. She did not require radiation therapy.
Perspective: T lymphoblastic lymphoma is a neoplasm of immature T-cells. It comprises about 2% of all lymphomas and it has an incidence of 2 per million in the pediatric age group. (1) Cardiac involvement is usually a late manifestation of lymphoma with symptoms such as congestive heart failure, arrhythmia, heart rupture, chest pain and dyspnea predominating. (2) Our patient, however, was remarkably asymptomatic from a cardiovascular standpoint. Furthermore, cardiac involvement of T cell lymphoma is not frequently reported in children except for those who underwent cardiac transplant. (3) Thus, this appears to be a quite unusual presentation of cardiac lymphoma. Although echocardiography was able to demonstrate cardiac involvement, it was limited in demonstrating extent of tissue infiltration. CMR better characterized tissue infiltration and provided further information regarding extent of cardiac involvement. As such, CMR should be considered in patients with suspected cardiac involvement of a malignancy in order to better define tissue infiltration.
References:
1. Cortelazzo S, Ponzoni M, Ferreri A, et al. Lymphoblastic lymphoma. Crit Rev Oncol Hematol. 2011;79:330-343.
2. Manabe M, Yoshii Y, Mukai S, et al. Precursor B-cell lymphoblastic lymphoma involving an intracardiac mass and myocardial infiltration: A case report. Intern Med. 2012;51:315-319.
3. Mahmoud R, Weitzman S, Schechter T, et al. Peripheral T cell lymphoma in children and adolescents: A single institution experience. J Pediatr Hematol Oncol. 2012;34(8):611-616.
COTW handling editor: M. Jay Campbell, MD
Have your say: What do you think? Latest posts on this topic from the forum