



Case from: Regitse H. Christensen*, Anne-Mette Leffers# MD, Jens Hove* MD PhD, and Per Lav Madsen* MD DMSc
Institute: The Cardiovascular MRI Unit, Depts. Radiology# and Cardiology*, Hvidovre University Hospital, Copenhagen University, Denmark
Clinical history:
A 33-year-old man was suspected of having a regurgitant quadricuspid aortic valve on the basis of transthoracic echocardiography following the incidental discovery of a diastolic murmur. The echo window, however, was suboptimal; cusp-opening, required to ensure a true quadricuspid valve morphology, could not be verified, and quantification of regurgitation was difficult with substantial inter-observer disagreements.
CMR Findings:
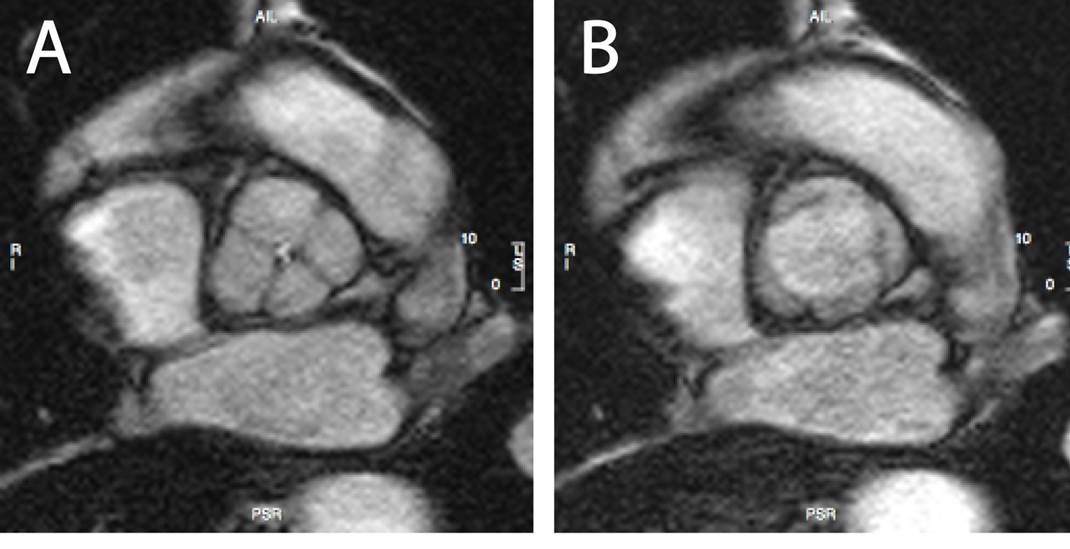
Figure 1A & 1B: Hurwitz and Roberts type A quadriscuspid valve in diastole and systole, respectively
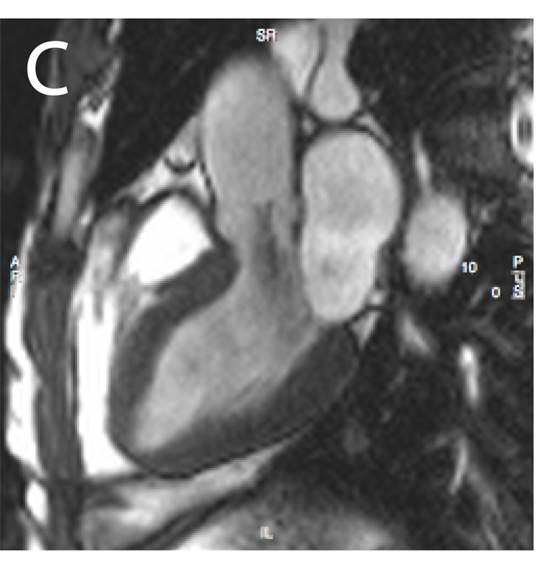
Figure 1C: 3-Chamber view showing the aortic regurgitation
Cardiac Magnetic Resonance (CMR) imaging confirmed a quadricuspid valve with four equal and fully separated cusps (Hurwitz and Roberts type A) and a central regurgitation orifice [Figures 1A, 1B & 1C].
Movie 1: Hurwitz and Roberts type A quadricuspid valve dynamics during the cardiac cycle
Movie 2: 3-chamber view, showing the central aortic regurgitation
The left ventricular end-diastolic and end-systolic volumes were 144mL and 42mL respectively (LVEF 71%, stroke volume 97 mL) [Movies 1-5].
Flow sequences demonstrated a regurgitant fraction of 13%, i.e. a mild aortic insufficiency.
CMR also allowed to rule out other potential concomitant structural defects.
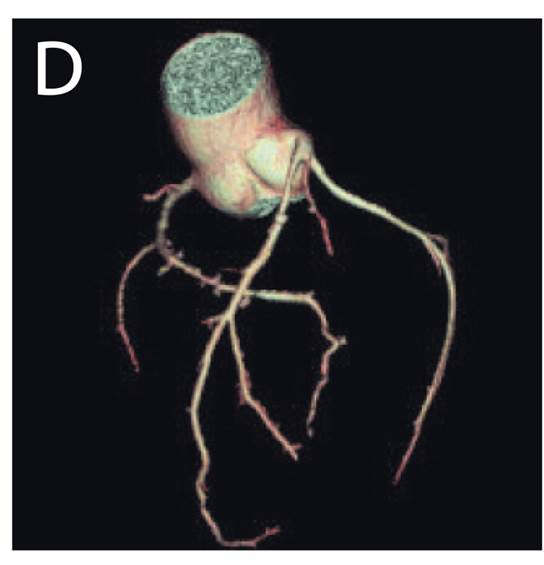
Coronary CT showed no aberrant coronary arteries [Figure 1D].
At follow-up 9 months later, CMR was repeated, and the regurgitant fraction was unchanged.
Conclusion:
This case accentuates the potential of modern cardiac imaging techniques in comprehensive aortic valve characterisation, and we now plan to follow this patient with regular cardiac MRI.
Perspective:
Quadricuspid aortic valves are rare congenital malformations and in most cases accompanied by both structural and dynamic defects. Of the 186 quadricuspid aortic valves reported from 1862 to 20041, 75% were insufficient and further 8% were both stenotic and insufficient. 18% had associated defects, most commonly an ASD or aberrant coronary arteries. 50% of patients required aortic valve replacement, often with patients in their 50s-60s.
CMR provides for a comprehensive aortic valve characterization with good prognostication of patients with regurgitant aortic valve lesions: patients with a regurgitant fraction <26% have a good prognosis and patients with a fraction >33% require valve replacement within a few years2.
Modern cardiac imaging techniques, including CMR, provides for comprehensive evaluation of regurgitant aortic valve lesions including characterization of the occasional rare regurgitant quadricuspid valve. Imaging of the valve is easy, and precise evaluation of left ventricular volume/dimensions and forward flow and regurgitant fraction is effortless and reproducible.
References:
1. Tutarel O. The quadricuspid aortic valve: a comprehensive review. J. Heart Valve Dis. 2004; 13:534–537.
2. Myerson SG, d’Arcy J, Mohiaddin R, Greenwood JP, Karamitsos TD, Francis JM, Banning AP, Christiansen JP, Neubauer S. Aortic Regurgitation Quantification Using Cardiovascular Magnetic Resonance: Association With Clinical Outcome. Circulation. 2012; 126:1452–1460.
COTW handling editor: Monica Deac

