



Case from: Kae Watanabe1, Kurt Scherer2, Arun Chandran 1,2,3
Institute: 1 Department of Pediatrics, University of Florida, Gainesville, FL, U.S.A.; 2 Department of Radiology, University of Florida, Gainesville, FL, U.S.A.; 3 UF Health Congenital Heart Center, University of Florida, Gainesville, FL, U.S.A.
Clinical History:
An asymptomatic 3 year old was evaluated for a murmur. Physical examination was significant for a widely split second heart sound with an ejection systolic murmur in the left upper sternal border. An initial chest X-ray (Figure 1) was suggestive of a significant left to right shunt with cardiomegaly, increased pulmonary vascular markings and hyperinflation of the alveolar fields. A transthoracic echocardiogram (TTE) was highly suggestive of an inferior sinus venosus atrial septal defect (IVC-ASD) with questionable anomalous drainage of the right lower pulmonary vein into the right atrium. A confirmatory cardiac magnetic resonance imaging was performed under general anesthesia with breath holding.
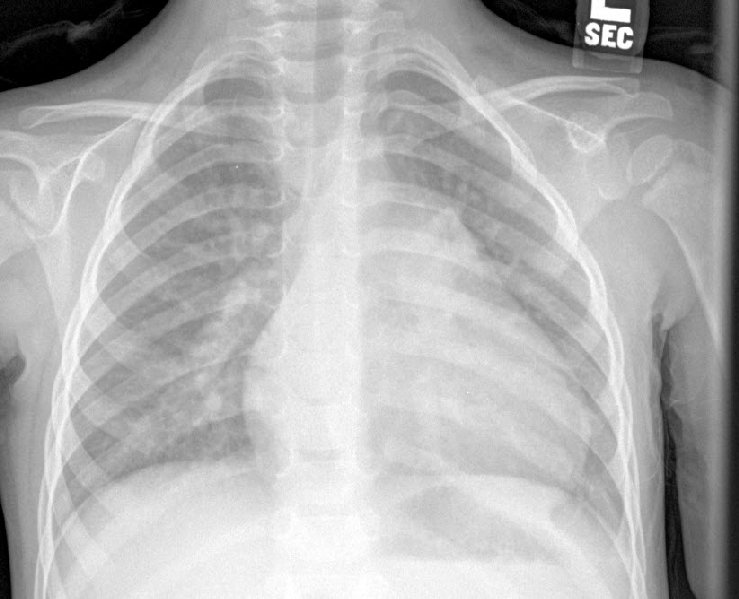
Fig 1
CMR Findings:
The CMR images confirmed the presence of a rare inferior sinus venosus type of ASD (Movie 1,2) with significant left to right shunting (QP/ QS: 3.4: 1 based on Phase contrast Imaging). There was severe right heart dilation (Right ventricular end-diastolic of: 195ml/m2 (normal 47 – 103 ml/m2) Z-score : 8.67. The RV end-systolic volume indexed was 83ml/m2 with normal RV EF of 57%). There was demonstrable over-riding of the inferior vena cava and the corresponding angiogram (Movie 3)) demonstrated partial anomalous pulmonary venous drainage of the right lower pulmonary vein into the inferior vena cava close to its junction with the right atrium as demonstrated by the arrow in 3D reconstruction (Figure 2A and 2B) . These findings were also present on the pre-operative trans-esophageal echocardiogram (TEE) (Movie 4 and 5).


Movie 1 & Movie 2
Movie 1: MRI short-axis plane showing dilated right ventricle with clearly demonstrated inferior sinus venosus atrial defect and associated over-riding of the inferior vena cava
Movie 2: MRI horizontal long –axis view showing posteriorly located sinus venosus ASD with right heart dilation and right ventricular hypertrophy
Movie 3
Movie 3: Magnetic resonance Angiography sequence demonstrating anomalous drainage of the right lower pulmonary vein to the junction of the inferior vena cava and the right atrium

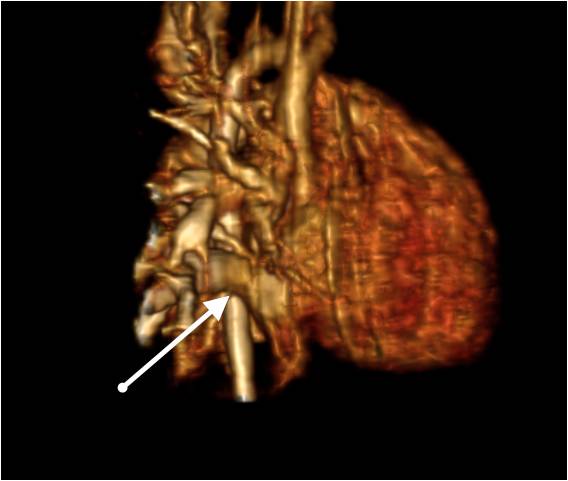
Fig 2A & Fig 2B
Figure 2A and 2B: MPR and 3D volume rendered reconstruction from the MRA with arrow pointing drainage of RLPV to the IVC

Movie 4 & Movie B
Movie 4: TEE simultaneously demonstrating presence of a large defect in the posterior aspect of the atrial septum with left to right flow
Movie 5: TEE 4 chamber view showing moderate right heart dilation secondary to the left to right shunt
Conclusions:
She underwent successful patch closure of the atrial septal defect with re-routing of the right lower pulmonary vein to the left atrium. Sinus venosus atrial septal defects are rare and the inferior variety is even less frequently seen as compared to the superior type. This case describes such a unique entity and demonstrates the singular ability of cardiac magnetic resonance imaging to diagnose the lesion qualitatively and in addition provides quantitative information on it’s hemodynamic consequences.
Perspective :
Arial septal defects occur in about 1.5 per 1,000 newborns. Caval vein defects are the least common forms of atrial communications forming only 2-10% of all inter-atrial communications (1). The superior form of caval vein defects constitute the majority and also the most well recognized type while the IVC-ASD, also known as “Right atrial type SVD”, is rare with only case reports and small case series published(2). In contrast to primum or secundum atrial septal defects, IVC-ASD do not typically involve the septum primum or the valve of the fossa ovale (2). In an inferior SVD, the inter-atrial communication extends into the IVC outside the confines of the atrial septum, making device closure difficult (3). Furthermore as a result of this abnormal defect, the IVC overrides the defect with associated potential for abnormal pulmonary venous return, typically an anomalous right lower pulmonary vein(3). The embryological etiology of this defect is incomplete absorption of the sinus venosus into the main chamber of the right atrium.
Traditional diagnostic tests included TTE, TEE and cardiac catheterization. TTE can provide the information necessary for surgical planning in the majority of cases, unfortunately it is hard to obtain a good acoustic window at times as the defect is located posteriorly (4)(5). TEE is an excellent alternative and is proven to diagnose defects that are important in diagnosing. The disadvantages include the semi-invasive nature and limited ability to image extra-cardiac structures. Cardiac catheterization can be used for evaluation, however radiation and the invasive nature are drawbacks. In the current period, CMR remains the gold standard in the evaluation of such rare defects due to their ability to provide the physician information related to the location and size of the defect as well as secondary hemodynamic burden in the form of QP/QS determination as well as volumetric and functional information. CMR provides the surgeon the best road-map for a successful and complication-free operation (6).
References:
1.Tomar M, Radhakrishnan S, Kaushal SK, Dagar KS, Iyer KS, Shrivastava S. Inferior-type caval vein defect–echocardiographic and surgical description of a large series of patients. Cardiology in the Young 2012 Jun;22(3):270-8.
2.Banka P, Bacha E, Powell AJ, Benavidez OJ, Geva T. Outcomes of inferior sinus venosus defect repair. The Journal of Thoracic and Cardiovascular Surgery 2011 Sep;142(3):517-22.
3.Plymale J, Kolinski K, Frommelt P, Bartz P, Tweddell J, Earing MG. Inferior sinus venosus defects: anatomic features and echocardiographic correlates. Pediatric Cardiology 2013 Feb;34(2):322-6.
4.Oliver JM, Gallego P, Gonzalez A, Dominguez FJ, Aroca A, Mesa. Sinus venosus syndrome: atrial septal defect or anomalous venous connection? A multiplane transoesophageal approach. Heart. 2002 Dec;88(6):634-8.
5.Crystal MA, Najashi KA, Williams WG, Redington AN, Anderson RH. Inferior sinus venousus defect: Echocardiographic diagnosis and surgical approach. Congenital Heart Disease J Thorac Cardiovasc Surg. 2009; 137(6):1349-55.
6.Valente AM, Sena L, Powell AJ, Del Nido PJ, Geva T. Cardiac magnetic resonance imaging evaluation of sinus venosus defects: comparison to surgical findings. Pediatric Cardiology 2007 Jan-Feb;28(1):51-6.
COTW handling editor: Vikas K. Rathi, MD
Have your say: What do you think? Latest posts on this topic from the forum