



Case from: Elisabetta Chiodi1, Maria Teresa Cannizzaro1, Bruna Malta2, Clorinda Montalto2, Zairo Ferrante2, Marcello Natali2, Andrea Fiorencis3, Donato Mele3, Giorgio Benea1.
Institute: 1) Radiology Department, 2) University Radiology Department, 3) Cardiology Department. Arcispedale Sant’ Anna, Cona (Ferrara), Italy
Clinical history:
A 75-year-old Caucasian female, diagnosed with intestinal carcinoid tumor 6 years previously, presented with a syncopal episode. Her ECG was negative (Image 1). Echocardiography showed a pseudonodular thickening of the mid-basal lateral wall of the left ventricle without regional wall motion abnormalities (Movie 1).
She was referred to our CMR department for better evaluation of the cardiac mass.

Image 1
Movie 1
CMR Findings:
Cine MRI (Movie 2, 3) confirmed the presence of the nodular lesion and showed normal LV global and regional function.

Movie 2 and Movie 3
On T1-weighted spin echo sequences the intra-myocardial mass in the antero-lateral LV wall had moderate signal intensity (Image 2); on T2-weighted spin echo and STIR images (Image 3) the mass showed a high signal intensity, while on SSFP images the lesion appeared inhomogeneous.
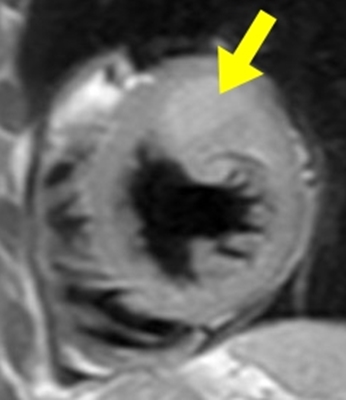
Image 2- T1W

Image 3 – T2W
Late Gadolinium images showed an extensive delayed enhancement within the mass (Image 4).

Image 4 – Late Gadolinium Enhancement
There was mild pericardial effusion but there was no evidence of pericardial involvement.
Subsequently the patient underwent a whole-body octreotide scintigraphy (Image 5a, 5b) that showed focal enhancement in the left thoracic base at the level of the LV lateral free wall. No explanation was found to the syncopal episode, which was therefore considered as an incidental finding.
The patient underwent ileocolectomy at presentation 6 years previosly. Following the finding of cardiac metastatis, patient was treated with a somatostatin analogue drug (octeotide).
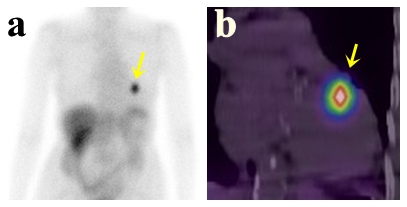
Image 5 a/b. Whole-body octreotide scintigraphy
Clinical history, laboratory tests, echocardiogram and CMR suggested the diagnosis of cardiac metastases from carcinoid tumor [1]. A total body CT and octreotide scintigraphy showed no other organ involvement from the carcinoid.
Perspective:
Carcinoid tumors are a slow-growing type of neuroendocrine tumor, originating from enterochromaffin cells [1]. The most common tumors are from bronchus-pulmonary or gastro-intestinal tracts, neuroendocrine tumors can arise from almost any organ. These tumors are relatively uncommon, with an average annual incidence of 1.00/100000 and 0.70/100000 for men and women respectively [1]. Cancer cells contain peptides and amines and can secrete serotonin, bradykinins, tachykinins, peptide A, ACTH, histamine. These substances are responsible for carcinoid syndrome that occurs in less than 10% of patients with carcinoid tumors. The syndrome consists of cutaneous flushing, sweating, bronchospasm, colicky abdominal pain, and diarrhoea. Approximately 55% of patients with carcinoid syndrome develop a carcinoid heart disease, mostly affecting the right heart (in particular causing tricuspid valve stenosis or insufficiency) [2-4]. A small pericardial effusion can be present [5]. Carcinoid syndrome is frequently associated with metastasis, most commonly in the liver.The incidence of myocardial metastasis is approximately 4%; the right ventricle is involved in 40% of the cases, the left ventricle in 53% and the ventricular septum in 7%.; rarely the pericardium [6, 7] or a left atrium are involved. Cardiac carcinoid metastases can mimic benign cardiac tumors (e.g., myxoma) or valvular abnormalities, often seen in patients with carcinoid syndrome. Diagnostic imaging plays a pivotal role in the initial assessment of carcinoid tumors and in monitoring their response to therapy [8]. Echocardiography represents the first diagnostic step. Usually the majority of metastatic lesions are seen by echo as limited, non-infiltrating and homogeneous masses[9]. CMR is a fundamental imaging modality in the diagnostic work-up, with improved detections of the lesions, given its high spatial, temporal, and contrast resolution, free choice of image plane and image size, myocardial motion and perfusion assessment; in addition CMR can accurately evaluate the relationship among pericardial, pulmonary, or mediastinal masses and the heart [10]. Carcinoid metastases have inhomogeneus signal intensity on SSFP images, intermediate signal intensity on T1-weighted spin echo sequences and high signal intensity on proton density, T2-weighted spin echo and STIR sequences. Carcinoid metastases usually show contrast enhancement during rest perfusion [7]. Our case shows the clinical role of CMR in the diagnostic work-up of cardiac masses, and in particular when carcinoid metastases are suspected.
References:
1) Efren Martinez-Quintana, Maria Del Mar Avila-Gonzalez, Laura Suarez-Castellano, Fayna Rodriguez-Gonzalez. Metastatic carcinoid tumor presenting as right sided heart failure. Int J Endocrinol Metab. 2013;11:120-125
2) Jonathan Meurice, Stéphane Boulé, Guillaume Deswarte, François Brigadeau, Thomas Modine. Solitary atrial myocardial metastasis revealing ileal neuroendocrine carcinoma. Cardiovascular Pathology 2012;21:355–357
3) Patricia A. Pellikka, A. Jamil Tajik, Bijoy K. Khandheria, James B. Seward, John A. Callahan, Henry C. Pitot, Larry K. Kvols. Carcinoid heart disease. Clinical and echocardiographic spectrum in 74 patients. Circulation. 1993;87:1188-1196
4) George S. Chrysant, Douglas A. Horstmanshof, Uma M. Guniganti. Metastatic carcinoid tumor obstructing left ventricular outflow. Tex Heart Inst J. 2011;38:282-4
5) Lee S, Lee SP, Sohn DW. Diffuse myocardial metastasis of carcinoid tumour. Heart. 2014 Mar;100:438-9.
6) Collins N, Bellamy G, Hayes P. Intrapericardial carcinoid metastasis. J Am Soc Echocardiogr. 2004;17:675-6.
7) M Puvaneswary, D Thomson, GR Bellamy. Cardiac metastasis from carcinoid tumour: Magnetic resonance imaging findings. Australasian Radiology 2004;48:383–387
8) Marcus D. Seemann, Jochen Gaa. Cardiac metastasis visualization with Positron Emission Tomography, Computed Tomography, Magnetic Resonance Imaging, Positron Emission Tomography/Computed Tomography, and Positron Emission Tomography/Magnetic Resonance Imaging. Circulation 2005;112:e329-e330
9) Utpal H. Pandya, Patricia A. Pellikka, Maurice Enriquez-Sarano, William D. Edwards, Hartzell V. Schaff, Heidi M. Connolly. Metastatic carcinoid tumor to the heart: echocardiographic-pathologic study of 11 patients. Journal of the American College of Cardiology. 2002, 40:1328-32
10) Bogaert J., Dymarkowski S., Taylor A.M., Muthurangu V. Cardiac masses in Clinical cardiac MRI, Springer. 2012;411-439