



Case From: Jason Craft MD, Subha Raman, MD, MSEE
Institute: Ohio State University, Columbus, Ohio
Clinical history:
A 70 year-old male had presented approximately 6 months prior to another hospital with fatigue, weakness, chest pain and dyspnea. At that time, left heart catheterization showed non-obstructive coronary artery disease and elevated left ventricular end-diastolic pressures with a restrictive filling pattern. An echocardiogram demonstrated increased biventricular wall thickness, and the left ventricular ejection fraction was estimated to be 55-60%. He underwent abdominal fat pad biopsy that showed apple green birefringent crystals on congo red staining. Elevated lambda free light chains were detected in the serum. He transferred his care to our institution for cardiac and oncology management.
Diagnostic Testing:
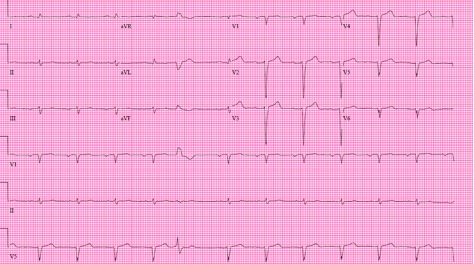
Figure 1. EKG: Normal sinus rhythm with rare PVC, pseudoinfarct pattern in anteroseptal leads, first degree AV block
CMR Findings: .
a) GRAPPA cine in the HLA, VLA, and SAX planes (movies 1-3) performed due to arrhythmia and inability to hold breath (FOV 305 X 420 mm, matrix 90 X 160, voxel size 3.3 X 2.6 mm, TR 65.4 ms, TE .9 ms, steady-state free precession readout). There is severe biventricular dysfunction, mild left ventricular hypertrophy, with a LVEF measured at 25% by area-length formula.
Movie 1. GRAPPA cine in Horizontal Long Axis (HLA) View.

Movie 2. GRAPPA cine in Vertical Long Axis (VLA) View.
Movie 3. GRAPPA cine in Short Axis (SAX) View.
b) PSIR single-shot acquisitions from the VLA and short axis planes (FOV 298 X 450 mm, matrix 127 X 192, voxel size 2.3 X 2.3 mm, TI 400 ms, TE 1.0 ms, TR 820 ms, TruFISP readout) (Figure 1). There is demonstration of thrombus in the left atrial appendage (arrow). There was inability to null the myocardium, which is consistent with cardiac amyloidosis. The extracelluar volume (ECV) calculated using pre and post contrast MOLLI sequences was 80% of the myocardium1.
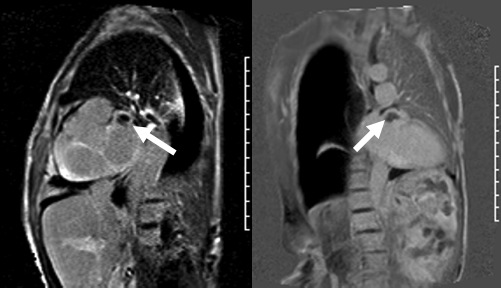
Figure 2. PSIR single-shot acquisitions from the short axis and VLA planes
Conclusion:
The final diagnosis was AL (primary) amyloidosis and smoldering multiple myeloma with cardiac involvement. Treatment was started with CYBord (velcade, cytoxan, dexamethasone). Enoxaparin therapy was started for the left atrial appendage thrombus. Given major cardiac involvement, and a clinically estimated 5 yr overall survival of 40%, ICD implantation for primary prevention was not recommended.
Perspective:
Several key findings of cardiac amyloidosis were identified in this study. Atrial fibrillation is common in this population, for which real-time cine imaging was helpful. CMR has not gained widespread use for LAA thrombus detection, despite prior reports suggesting high sensitivity and specificity. This may be attributable to the overall low incidence of thrombus in study populations comparing CMR to transesopohageal echocardiography2. With the addition of three dimensional contrast MRA, which was not performed in this study, detection may approach that of transesophageal echocardiography. 100% concordance between CMR and TEE for the diagnosis of left atrial appendage thrombus has been described when pulmonary vein MR angiography was used as the source images in patients undergoing pulmonary vein isolation (PVI)2. It may be a reasonable approach to interrogate the left atrial appendage for thrombus in instances of high clinical suspicion.
References:
1. Kellman P, Herzka DA, Arai AE, Hansen MS. Influence of Off-resonance in Myocardial T1-mapping using SSFP based MOLLI Method. J Cardiovasc Magn Reson. 2013 Jul 22;15:63
3. Rathi et al. Contrast-enhanced CMR is equally effective as TEE in the evaluation of left atrial appendage thrombus in patients with atrial fibrillation undergoing pulmonary vein isolation procedure. Heart Rhythm 2013 Jul;10(7):1021-7
COTW handling editor: Lilia Sierra-Galan, MD

