



Mahi L. Ashwath MD, MBA, FACC, FASE, FSCMR, Tommy Robinson MD
University of Iowa Hospitals and Clinic, Iowa City, Iowa, 52246
Case Published in the Journal of Cardiovascular Magnetic Resonance: Click here for the link
Click here for PubMed Reference to Cite this Case
Clinical history
A 52-year old female without prior medical history was admitted with Influenza A myocarditis progressing to cardiogenic shock. She eventually required extracorporeal membrane oxygenation for biventricular failure on multiple inotropic medications. Nine days into admission, she received implantation of a HeartMate II left ventricular assist device (LVAD) and was subsequently discharged. Over the next six months, myocardial function and clinical status improved. Her left ventricular (LV) ejection fraction on echo improved to 55-60%, with low LVAD speeds. Her LVAD was explanted.
One year later she experienced an isolated episode of transient double vision for a few minutes. An echocardiogram did not reveal a thrombus, but raised a suspicion of noncompaction and was felt to be of limited image quality. A cardiac magnetic resonance imaging (CMR) scan was performed to assess for non-compaction and thrombus formation.
CMR findings
Her CMR revealed normal right and left ventricular systolic function, and dyskinetic apical segments. The MRI scan also revealed a felt plug placed at the time of LVAD explantation. The felt plug was visualized as a mass at the LV apex measuring 5.2 cm in length, 1.6 cm in width on the localizer images. Two cm was contained within the LV cavity and 3.1 cm was present outside the LV cavity. The mass was isointense with the myocardium on steady state free precession cine images (Videos 1 and 2) and on T2 weighted turbo spin sequences (Figure 1).

| Video 1. 2-chamber SSFP | Video 2. 3-chamber SSFP |

Figure 1. Short-axis T2 weighted image depicting an isotense mass in the LV cavity.
It did not suppress with triple inversion fat suppression sequences (Figure 2) and did not perfuse with contrast on perfusion imaging (Video 3). On post-contrast high inversion time imaging the plug appears hypointense (Figure 3). On post contrast magnitude delayed enhancement imaging with an inversion time to null the myocardium, the felt plug had an etched appearance (Figure 4). On post contrast phase sensitive inversion recovery sequences, the felt plug was hypointense (Figure 5). Bright scar was present around the felt plug site, due to post-operative changes. As part of the clinical evaluation, the cardiac MRI did not reveal any evidence of non-compaction or obvious thrombus.
Video 3. 4-Chamber first pass perfusion.

Figure 2. Short-axis triple inversion fat suppression.
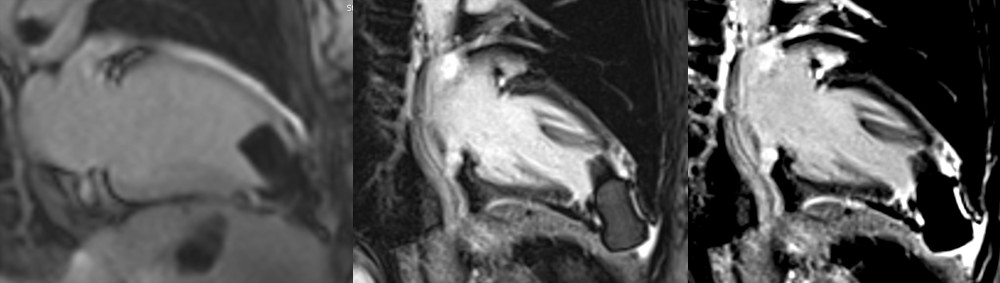
| Figure 3. LGE Long TI | Figure 4. LGE Magnitude | Figure 5. LGE PSIR |
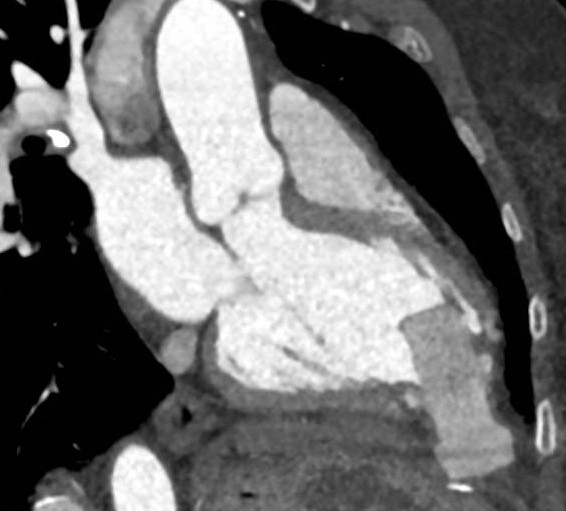
Figure 6. CT Features of Felt Plug used during LVAD Explantation.
| Sequence | Imaging Features |
| T2 weighted turbo spin sequence | Isointense |
| Post-contrast high inversion time imaging | Hypointense |
| Post contrast magnitude delayed enhancement imaging with an inversion time to null the myocardium | Hyperintense with an etched appearance |
| Post contrast phase sensitive inversion recovery sequence | Hypointense |
| Steady state free precession cine image | Isointense |
| Perfusion imaging | No perfusion |
Conclusion
To the best of our knowledge, this is the first report of MRI imaging of an LVAD felt plug. Although there wasn’t any metal artifact on the MRI imaging, to ensure patient safety for future scans, a Computed Tomography (CT) scan of the chest was performed (Figure 6).
With the expanding indications and increasing safety of LVADs, the implantation rates have increased. A small percentage of patients improve their function, leading to removal of the LVAD. Multiple approaches have been described for explantation, including primary closure, patch closure, titanium plug insertion, felt plug insertion and dividing the driveline and leaving the entire pump in situ (1). CMR studies in patients after LVAD explantation and primary closure reveal apical akinesis and tethering on cine imaging and apical scarring and transmural apical infarction on delayed enhancement sequences (2). Our case reports cardiac MRI findings and safety of felt plug imaging with CMR after LVAD explantation.
Perspective
Although the felt plug was not imaged by MRI in the past, it is MRI safe based on our study. Given the multiple approaches to explantation, it is important for MRI centers to review operative notes, X-rays, and any other imaging available in detail to assess for any metal remnants prior to scanning a patient after LVAD explantation. As there were concern of thrombogenicity of the plug remnants we discussed initiation of anticoagulation with surgeons and heart-failure specialists. Finally it was decided to not initiate anticogulation. There were no immediate or delayed complications from the procedure. While LVAD presence is an absolute contraindication for CMRI, these scans can be safely performed after explantation, even in the case of felt plug placement.
References
1. Selzman CH, Madden JL, Healy AH et al. Bridge to Removal: A Paradigm shift for Left Ventricular Assist Device therapy. Annals of Thoracic Surgery. 2015; 99(1):360-367
2. Moon JCC, Sievers B, Pennell DJ et al. Myocardial Scarring Caused by Left Ventricular Assist Device Insertion Demonstrated by Cardiovascular Magnetic Resonance. Journal of Cardiovascular Magnetic Resonance. 2003; 5(2), 361–363.
Click here to view the case on CloudCMR.
Case prepared by:
Pranav Bhagirath, MD PhD
Associate Editor
Amsterdam University Medical Center – Location VUmc, Amsterdam