



Hamidreza Pouraliakbar1, Mohammad Mahdavi1, Abdolmohammad Ranjbar1,2
1. Rajaie Cardiovascular, Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran
2. Cardiovascular research center, Tabriz University of Medical Sciences, Tabriz, Iran
Clinical History:
An eight-month-old boy with a history of recent coronavirus disease 2019 (COVID-19) infection (with positive real-time polymerase chain reaction test one month before presentation) was referred with symptoms of tachycardia, poor feeding, and respiratory distress. His symptoms for COVID-19 infection (one month before presentation) were mild fever, conjunctivitis, restlessness, and two other members from his family also tested positive for COVID-19. Conservative treatment had been considered for the patient due to his mild to moderate symptoms. The patient clinical and laboratory examinations revealed fever (39 Cº lasting more than 72 hours), faint friction rub, tachycardia, respiratory distress, and conjunctivitis as well as elevated C-reactive protein (CRP, 80 mg/L), elevated erythrocyte sedimentation rate (ESR, 90 s), serum Procalcitonin level of 1.25 ng/dl, D-dimer of 2.56 ng/dl, lactate dehydrogenase level of 1700 U/L, leukocytosis with 16700 white blood cells and 900 lymphocyte count, and elevated cardiac troponin I (cTnI) level (2.13 ng/dL; normal range <0.03 ng/dL). Symptoms of gastroenteritis including mild diarrhea and abdominal pain were also present. The patient was treated with a diagnosis of multisystem inflammatory syndrome in children (MIS-C) following COVID-19 with prednisolone, intravenous immune globulin (IVIG), and aspirin. In transthoracic echocardiography severe pericardial effusion, and moderately reduced left ventricular (LV) systolic function were detected (LV ejection fraction = 40%). After pericardiocentesis, the patients’ symptoms alleviated and Cardiovascular Magnetic Resonance (CMR) was performed.
CMR Findings:
CMR was performed at 1.5T (Siemens Avanto). Cine images revealed mild pericardial effusion and a giant aneurysm in the proximal segment of the left anterior descending artery (LAD, Movie 1, 2). Using T2-weighted imaging, myocardial edema was also depicted in CMR (Figure 1). Possible mid to epicardial late gadolinium enhancement in the basal anterior and inferolateral wall was evident (Figure 2).
Movie 1. Steady-state free precession (SSFP) cine coronal plane illustrating the large aneurysm of left anterior descending (LAD, green arrow) coronary artery next to the pulmonary artery. The giant aneurysm of the LAD has a comparable diameter to adjacent pulmonary artery.

Movie 2. Short axis SSFP cine illustrating giant aneurysm of the LAD. The giant aneurysm of the LAD can be seen in the interventricular groove (Red Arrow).

Figure 1. T2 weighted double inversion recovery four chamber with evidence of myocardial edema in the lateral left ventricular wall.
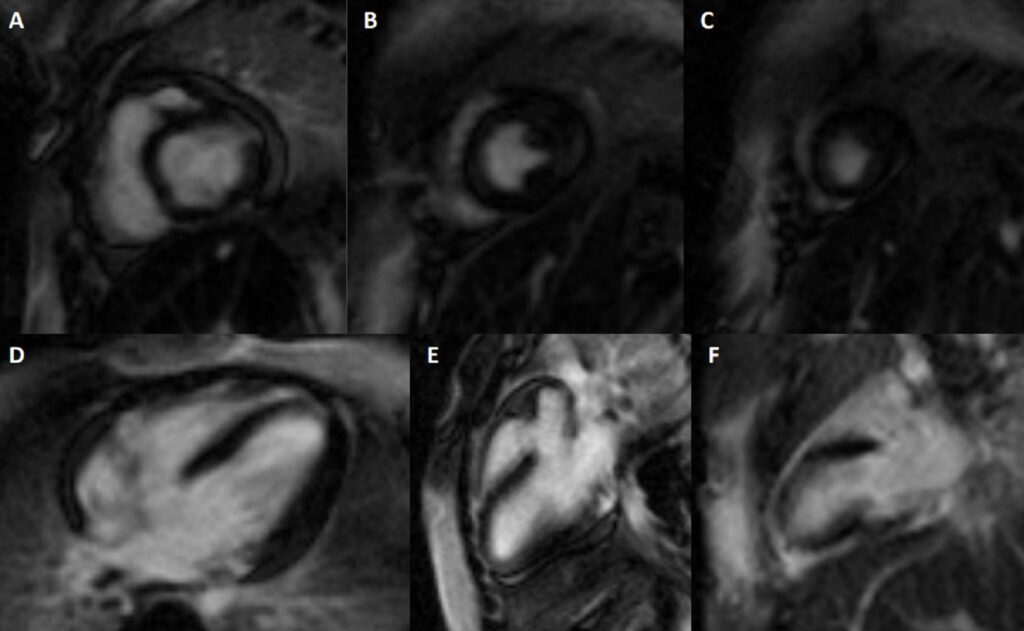
Figure 2. Possible mid to epicardial late gadolinium enhancement in the basal anterior and inferolateral wall was evident. A-C: Short axis stack. D-F: Four, three, two chamber.
Conclusion:
In order to visualize coronary aneurysm with possible clots and congenital anomalies in children based on the ward policy, the pediatric cardiologists ordered CT angiography in this case, confirming the aneurysmal dilation of the left main coronary artery (5 mm diameter), and multiple fusiform aneurysms in LAD with giant aneurysm at proximal portion (10 mm diameter) were depicted (Figure 3). Moreover, multiple fusiform aneurysms along the left circumflex coronary artery (LCX) (6.3 mm diameter) and fusiform dilation of origin of the right coronary artery (RCA) (3.7 mm diameter) were depicted (Movie 3).
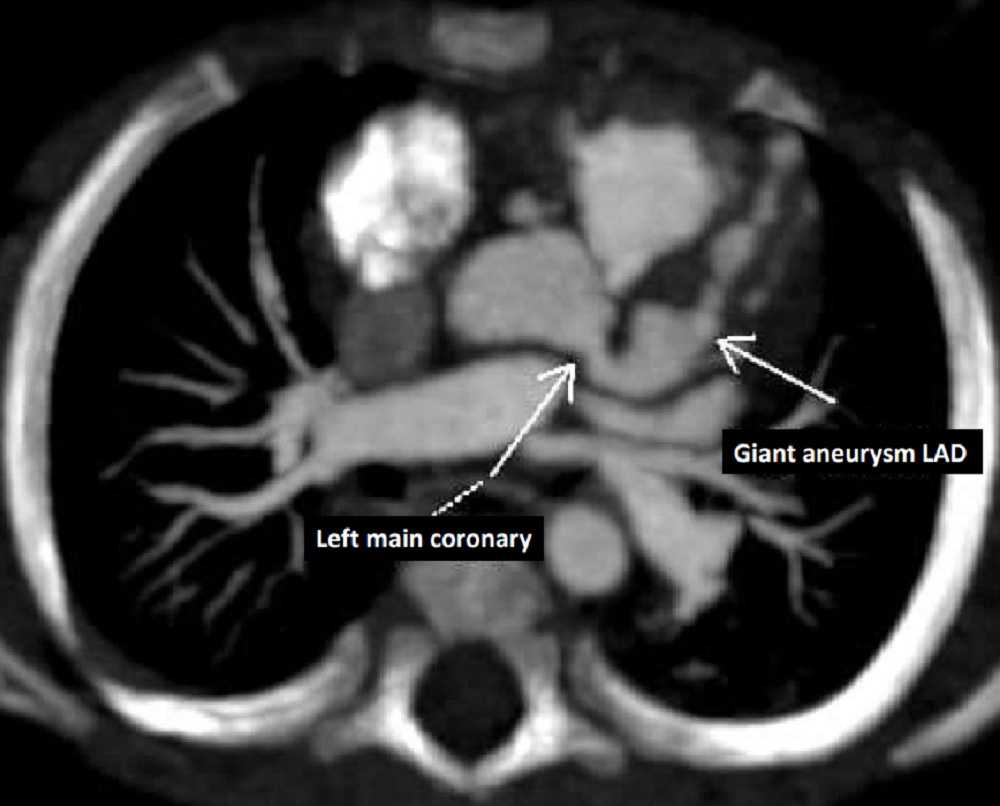
Figure 1. Axial image from the contrast-enhanced cardiac CT angiography shows aneurysmal dilation of the left main coronary artery at 5 mm diameter, and multiple fusiform aneurysms in the left anterior descending (LAD) coronary artery with a giant aneurysm (10 cm diameter) at the proximal portion were depicted.
Movie 3. Shaded surface display volume rendering (SS-VRT) creating a 3D visual illustration of CT volumetric data of the heart. Multiple fusiform aneurysms of coronary arteries are depicted.
Giant and widespread coronary artery aneurysms in an infant following COVID-19 infection is rarely reported in the literature; however, considering the possibility of fatal consequences, due regard should be given to this phenomenon. Moreover, previously the coronary artery aneurysms were depicted in magnetic resonance coronary angiography, nevertheless, in this case, giant coronary artery aneurysms were detected in CMR cine SSFP images. Subsequently treatment with infliximab, heparin, and warfarin was added to the patient’s treatment regime due to the coronary artery involvement resulting in partial response over two months, and the patient continues to be followed up.
Two recent studies using CMR imaging in adult patients after recovering from COVID-19 have reported cardiovascular abnormalities in 56 to 78% of middle-aged adults (9, 10). In another similar study, 15% of college athletes developed cardiovascular abnormalities in CMR imaging (11). In contrast, cohort studies on children using CMR for follow-up of the patients revealed fewer complications. Webster et al reported no significant cardiac disease by CMR in a small pediatric cohort of patients at least one month after recovering from acute symptomatic COVID-19 infection or MIS-C (12). Correspondingly, in another study after midterm follow-up (median of 7 months) in 16 children no patients had late gadolinium enhancement in CMR imaging (13). Blondiaux et al reported diffuse myocardial edema on T2 short tau inversion-recovery sequences and native T1 mapping in four children after MIS-C, with no evidence of late gadolinium enhancement (14).
Evidence is still scarce but rapidly emerging in the literature about the importance of performing CMR in patients with MIS-C. CMR can be considered as a safe and radiation-free substitute for evaluation of these patients – in particular the infants and children- and to identify myocarditis as well as functional abnormalities, and myocardial ischemia and infarction (15). CMR which is the mainstay in the diagnosis of suspected myocarditis helped us detect the myocarditis in our patient that would be missed if the workups were performed using other routine diagnostic modalities. Our case demonstrated the feasibility of detection of coronary artery aneurysm in CMR cine SSFP images, especially those with larger sizes. Therefore, due regard should be given to that the existence of possible coronary artery aneurysms not to be missed upon evaluation of cine SSFP images. Moreover, magnetic resonance angiography (MRA) can also be considered for the determination of the origin and course of coronary arteries in cases suspected of coronary artery disorders in children. Several studies advocate the accuracy of MRA in the detection of coronary artery aneurysms in patients with Kawasaki disease (16, 17). This technique can be regarded in such cases as a non-invasive and radiation-free imaging alternative when transthoracic echocardiography image quality is insufficient, subsequently reducing the need for serial x-ray coronary angiography.
References:
- Bellino S, Punzo O, Rota MC, Del Manso M, Urdiales AM, Andrianou X, et al. COVID-19 Disease Severity Risk Factors for Pediatric Patients in Italy. Pediatrics. 2020;146(4).
- Newburger JW, Takahashi M, Burns JC. Kawasaki disease. Journal of the American College of Cardiology. 2016;67(14):1738-49.
- Molaei A, Sadeghi-Shabestari M, Khomahani A, Ghaffari S, Sadat-Ebrahimi S-R. Cardiac biomarkers for early detection of cardiac involvement in children with Kawasaki disease: a cross-sectional study. International Journal of Pediatrics. 2019;7(12):10573-82.
- Sadat-Ebrahimi S-R. Diagnostic and Prognostic Value of Cardiac Biomarkers in Children with Kawasaki Disease: A State-of-the-Art Review. International Journal of Pediatrics. 2020;8(2):10911-28.
- Sarzaeim M, Rezaei N. Kawasaki Disease and Multisystem Inflammatory Syndrome in Children with COVID-19. SN Compr Clin Med. 2020:1-6.
- Toubiana J, Poirault C, Corsia A, Bajolle F, Fourgeaud J, Angoulvant F, et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. BMJ. 2020;369.
- Akca UK, Kesici S, Ozsurekci Y, Aykan HH, Batu ED, Atalay E, et al. Kawasaki-like disease in children with COVID-19. Rheumatology international. 2020:1-11.
- 8. WHO. Multisystem inflammatory syndrome in children and adolescents with COVID-19. 2021.
- Ng M-Y, Ferreira VM, Leung ST, Yin Lee JC, Ho-Tung Fong A, To Liu RW, et al. Patients recovered from COVID-19 show ongoing subclinical myocarditis as revealed by cardiac magnetic resonance imaging. Cardiovascular Imaging. 2020;13(11):2476-8.
- Puntmann VO, Carerj ML, Wieters I, Fahim M, Arendt C, Hoffmann J, et al. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA cardiology. 2020;5(11):1265-73.
- Rajpal S, Tong MS, Borchers J, Zareba KM, Obarski TP, Simonetti OP, et al. Cardiovascular magnetic resonance findings in competitive athletes recovering from COVID-19 infection. JAMA cardiology. 2021;6(1):116-8.
- Webster G, Patel AB, Carr MR, Rigsby CK, Rychlik K, Rowley AH, et al. Cardiovascular magnetic resonance imaging in children after recovery from symptomatic COVID-19 or MIS-C: a prospective study. Journal of Cardiovascular Magnetic Resonance. 2021;23(1):1-7.
- Barris DM, Keelan J, Ahluwalia N, Jhaveri S, Cohen J, Stern K, et al. Mid-Term Outcomes and Cardiac Magnetic Resonance Imaging Following Multisystem Inflammatory Syndrome in Children. J Pediatr. 2021.
- Blondiaux E, Parisot P, Redheuil A, Tzaroukian L, Levy Y, Sileo C, et al. Cardiac MRI in children with multisystem inflammatory syndrome associated with COVID-19. Radiology. 2020;297(3):E283-E8.
- Dietz SM, Tacke CE, Kuipers IM, Wiegman A, de Winter RJ, Burns JC, et al. Cardiovascular imaging in children and adults following Kawasaki disease. Insights Imaging. 2015;6(6):697-705.
- Greil GF, Stuber M, Botnar RM, Kissinger KV, Geva T, Newburger JW, et al. Coronary Magnetic Resonance Angiography in Adolescents and Young Adults With Kawasaki Disease. Circulation. 2002;105(8):908-11.
- Goo HW, Park I-S, Ko JK, Kim YH. Coronary CT angiography and MR angiography of Kawasaki disease. Pediatr Radiol. 2006;36(7):697-705.
Acknowledgement: Dr Seyyed-Reza Sadat-Ebrahimi
Case prepared by:
Jason N. Johnson, MD MHS
Associate Editor, SCMR Case of the Week
Le Bonheur Children’s Hospital, University of Tennessee Health Science Center, St. Jude Children’s Research Hospital