



Jyoti Gur, MD, Madhusudan Ganigara, MD, Waseem Cossor, MD
Division of Pediatric Cardiology, Department of Pediatrics, Advocate Christ Medical Center, Oak Lawn, IL, USA
Clinical History
A 25-year-old primigravida (G1P0) was referred at 22 weeks’ gestation for evaluation of a suspected fetal aortic arch abnormality identified on routine obstetric ultrasound. Initial fetal echocardiography demonstrated concern for interrupted aortic arch versus severe transverse arch hypoplasia with coarctation. It showed a well-developed left ventricular outflow tract (LVOT) with normal aortic valve (AV) dimensions, normal mitral valve (MV) annulus size, and normal left ventricular (LV) size and function. Additionally, there was normal right ventricular (RV) systolic function, cavity size, and wall thickness.
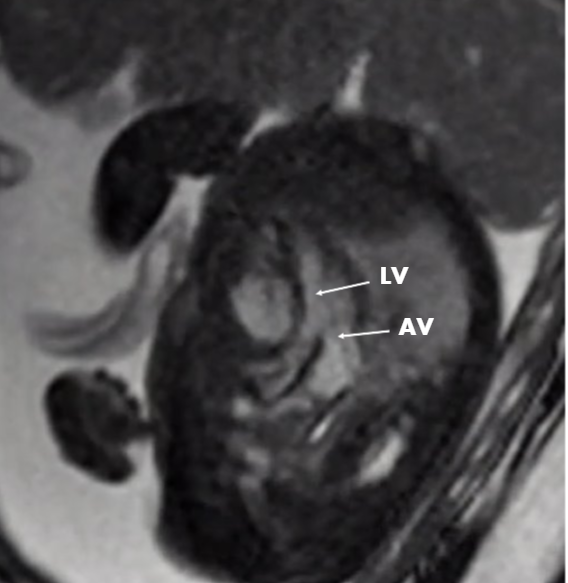
A follow-up fetal echocardiogram at 27 weeks’ gestation showed similar findings. However, a subsequent follow-up fetal echocardiogram at 30 weeks’ gestation demonstrated significant changes. New findings included supravalvar aortic stenosis (AS) (Figure 1), a highly tortuous distal ascending aorta and proximal transverse arch with antegrade flow throughout, and a narrowed, tortuous ductus arteriosus with increased velocity, consistent with premature ductal constriction (Figure 2). There was new moderate-to-severe dilation and hypertrophy of the RV with severely depressed global systolic function, as well as new mild-to-moderate tricuspid regurgitation (TR). LV size and systolic function remained normal throughout (Movies 1-3).
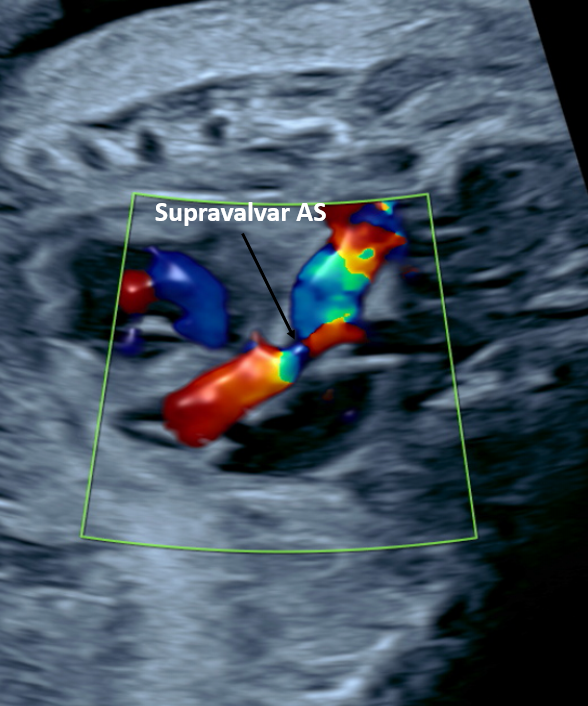 |
| Figure 1. Fetal echocardiogram demonstrating supravalvar AS with narrowing immediately above the AV in the LVOT. |
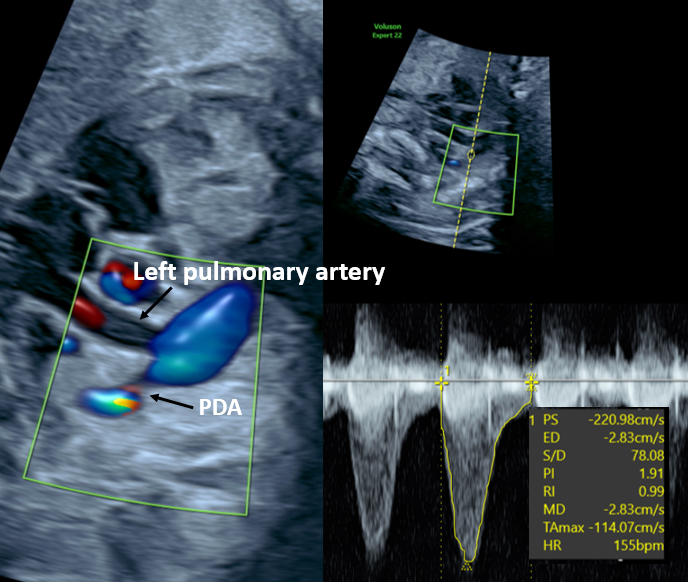 |
| Figure 2. Fetal echocardiogram demonstrating a narrowed, tortuous ductus arteriosus with increased Doppler velocity, consistent with premature ductal constriction. Patent ductus arteriosus (PDA). |
 |
| Movie 1. Fetal echocardiogram in the apical four-chamber view demonstrating new moderate-to-severe RV dilation and hypertrophy with severely depressed global systolic function, alongside preserved LV size and systolic function. |
 |
| Movie 2. Fetal echocardiogram demonstrating a highly tortuous distal ascending aorta and proximal transverse arch with antegrade flow throughout. |
 |
| Movie 3. Fetal echocardiogram with color Doppler demonstrating a narrowed, tortuous ductus arteriosus with increased velocity, consistent with premature ductal constriction. |
There was uncertainty regarding arch sidedness, level of obstruction, and brachiocephalic branching pattern, all of which would have significant postnatal management implications. Therefore, fetal cardiovascular magnetic resonance imaging (CMR) was performed at 30 weeks’ gestation to further delineate the anatomy.
CMR Findings
Fetal CMR was performed on a 1.5 T MAGNETOM Sola scanner (Siemens Healthineers, Erlangen Germany) using a 32-channel phased array torso coil placed on the maternal abdomen. For fetal cardiac gating, a MR-compatible DUS sensor (smart-sync, North Medical GmbH, Hamburg, Germany) was positioned on the woman’s abdomen and fixed with an elastic band. Sequences performed included compressed-sense 8-shot cine sequence in multiple long- and short-axis planes. The following parameters were used in the cine sequence: field of view 360 mm, flip angle: 80 degrees, echo time (TE): 1.39 ms, and slice thickness: 5.0 mm. additionally phase-contrast velocity encoding, and T2-weighted black-blood sequences were acquired in multiple overlapping stacks in fetal axial, coronal, sagittal, and oblique planes. Total scan time was 60 minutes. Slice-to-volume registration (SVR) was applied for motion correction, realigning individual slices into a high-resolution three-dimensional isotropic volume. Post-processing and multiplanar reformatting were performed using cvi42 (Circle Cardiovascular Imaging, Calgary, Alberta, Canada), and segmentation and virtual reality visualization was performed using Elucis software (Realize Medical, Ottawa, Ontario, Canada).
Fetal CMR revealed the following findings: a qualitatively normal-sized LV with a normal LVOT; a qualitatively dilated RV with depressed systolic function and a structurally normal right ventricular outflow tract (RVOT) without evidence of obstruction; and normal functioning mitral and tricuspid valves (Figure 3, Movies 4-6).
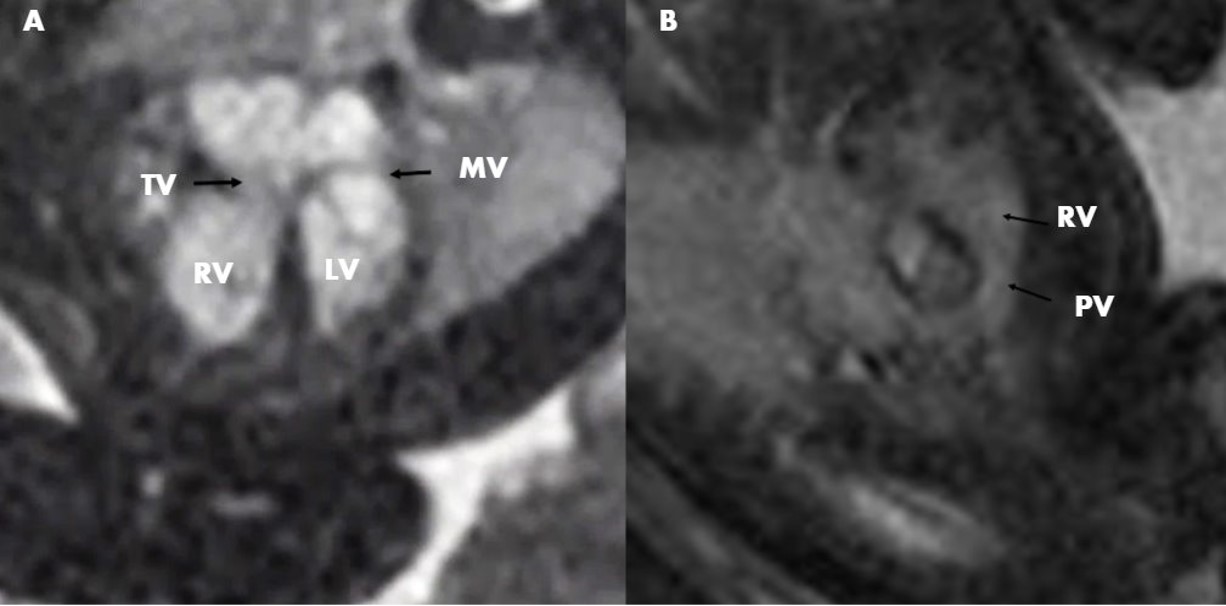 |
| Figure 3. Fetal CMR balanced steady state free precession (bSSFP) in the four-chamber (A) and RVOT (B) planes demonstrating qualitatively normal LV size, qualitatively dilated RV, and a structurally normal RVOT without evidence of obstruction. |
 |
| Movie 4. Fetal CMR bSSFP cine in the four-chamber plane demonstrating qualitatively normal LV size and function, with moderate-to-severe RV dilation and depressed systolic function. |
 |
| Movie 5. Fetal CMR bSSFP cine in the LVOT plane demonstrating a normal-sized AV and unobstructed LVOT, with dephasing artifact in the ascending aorta suggestive of supravalvar AS. |
 |
| Movie 6. Fetal CMR bSSFP cine in the RVOT plane demonstrating a qualitatively dilated RV with depressed systolic function and a structurally normal, unobstructed RVOT. |
There was a normal-sized AV with normal aortic root dimensions (Figure 4).
 |
| Figure 4. Fetal CMR bSSFP in the LVOT plane demonstrating a normal-sized AV and normal LVOT without evidence of obstruction. |
Supravalvar AS was suggested by dephasing artifact in the ascending aorta. There was a severely tortuous distal ascending aorta with an elongated and tortuous left aortic arch demonstrating moderate hypoplasia, as well as tortuosity of all brachiocephalic branch vessels. The distal arch and proximal descending aorta followed an elongated S-shaped course in the left thorax; transverse arch 3 mm, distal aortic arch 4.5 mm, proximal descending aorta 4.8 mm, descending aorta at the diaphragm 5.6 mm (Figure 5). Additionally, fetal CMR confirmed a moderate sized ductus arteriosus with discrete narrowing at the distal end, inserting into the hypoplastic transverse arch segment (Figure 6).
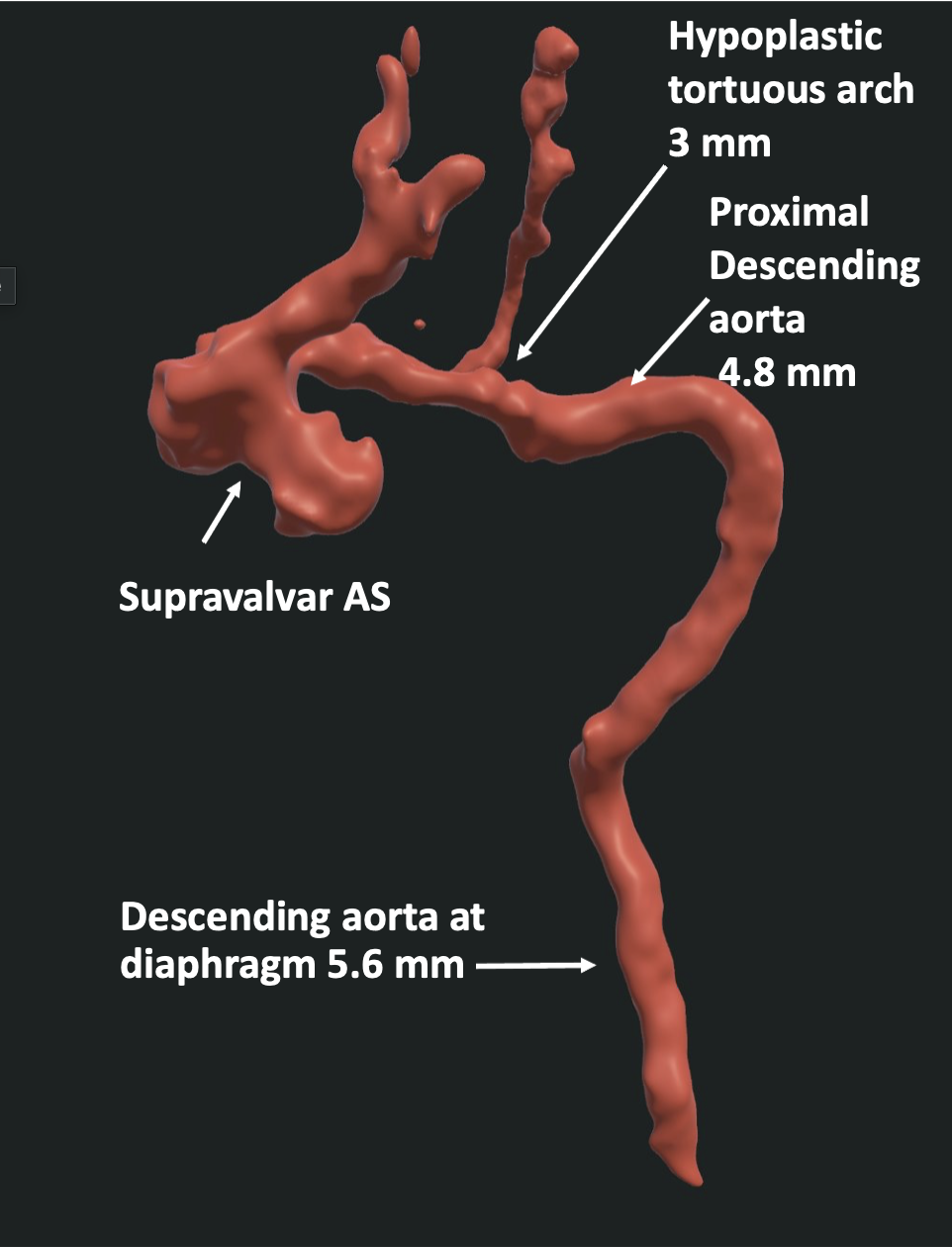 |
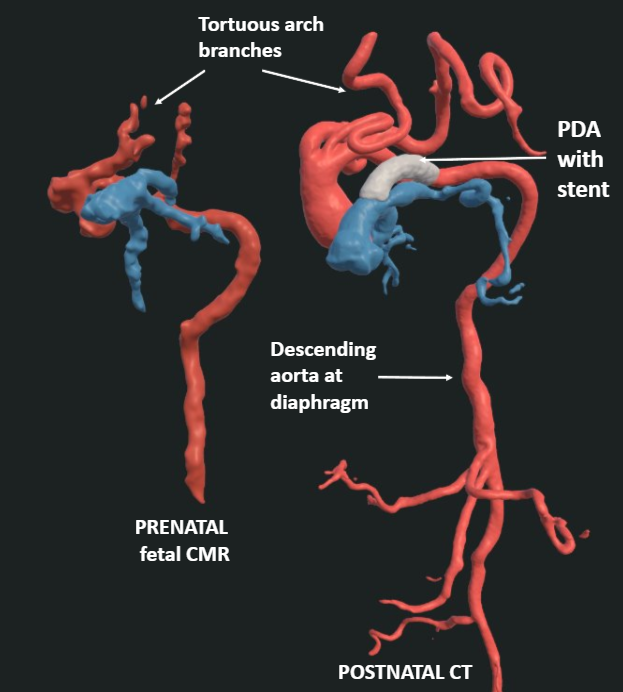
| Figure 5. Three-dimensional reconstruction following SVR demonstrating a severely tortuous, elongated aortic arch with moderate transverse arch hypoplasia. The distal arch and proximal descending aorta follow an elongated S-shaped course in the left thorax, with tortuosity extending into all brachiocephalic branch vessels. Arch continuity is definitively established, excluding interrupted aortic arch. |
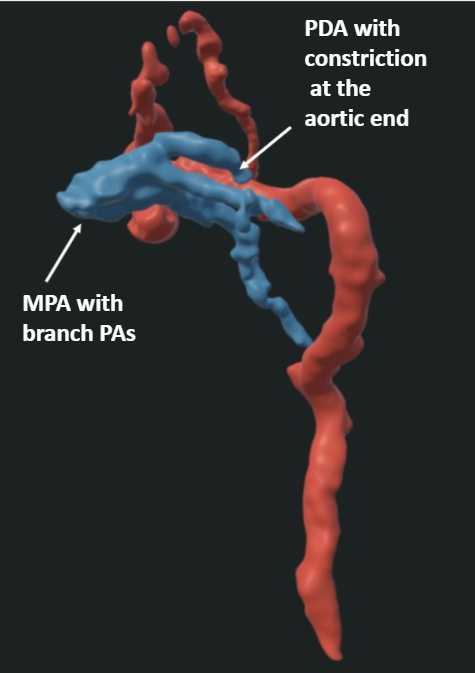 |
| Figure 6. Three-dimensional reconstruction demonstrating a moderately sized PDA with focal distal narrowing at its insertion into the hypoplastic transverse arch, consistent with premature ductal constriction. Blue color represents pulmonary arteries (PA) and PDA and red represents aorta. |
Conclusion
Fetal CMR demonstrated a severely tortuous but continuous aortic arch, definitively excluding interrupted aortic arch and establishing extreme arch tortuosity with an atypical course in the left thorax, transverse arch hypoplasia, and supravalvar AS as the primary aortic abnormalities. Additionally, the presence of marked tortuosity in the brachiocephalic branches and the atypical shape and course of the descending aorta raised concern for systemic arteriopathy. These findings were critical in guiding perinatal management toward postnatal prostaglandin E1 infusion and planning a catheter-based palliation. After a multidisciplinary clinical conference with maternal fetal medicine, neonatology, fetal cardiology, interventional cardiology, cardiothoracic surgery teams and detailed discussion with parents, it was decided to proceed with delivery at 32 weeks’ gestation. The main reason for this decision was progressive ductus arteriosus restriction demonstrated by both fetal echocardiography and fetal CMR, resulting in severe RV dilation and severe RV systolic dysfunction. Given the severity of RV dysfunction, the team predetermined that immediate ductal stenting would be pursued after delivery to provide RV decompression if feasible.
The infant was delivered via cesarean section at 33 weeks’ gestation, with birth weight of 2.6 kg; prostaglandin E1 infusion was initiated immediately at birth. The first postnatal transthoracic echocardiogram (TTE) was consistent with the fetal imaging findings and showed severe RV dysfunction, and severe ductal restriction (Movies 7-8). Initial postnatal supravalvar aortic gradient was 14 mmHg, and peak aortic isthmus gradient was 33 mmHg. The relatively low supravalvar gradient was underestimated because of downstream obstruction at the level of the aortic isthmus. The neonate subsequently underwent cardiac catheterization with ductal stent placement at 3 hours of life (Figure 7).
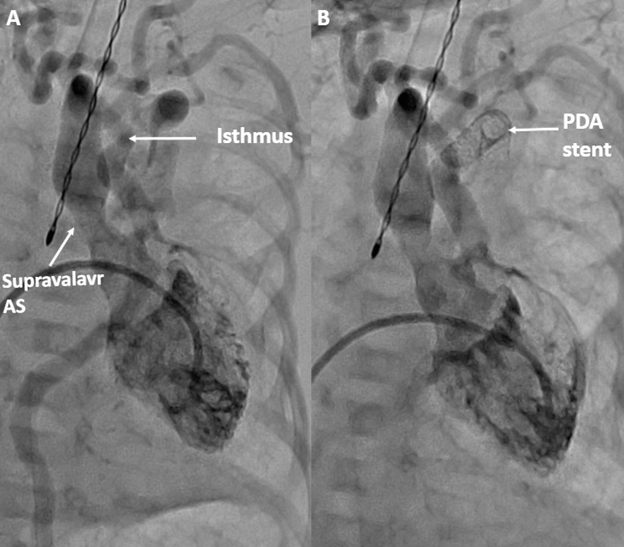 |
| Figure 7. Fluoroscopic angiogram obtained during cardiac catheterization at 3 hours of life before (A) and after (B) PDA stent angioplasty, delineating aortic arch and ductal anatomy to guide stent placement. |
 |
| Movie 7. Postnatal TTE in the apical four-chamber view demonstrating severe RV dysfunction, consistent with prenatal fetal imaging findings. |
 |
Movie 8. Postnatal TTE in the parasternal short-axis view demonstrating severe RV dysfunction amidst severe ductal restriction.< |
The fetal CMR showed the anatomy well enough that interventional cardiologists could plan their catheter-based approach. There was uncertainty based on the fetal echo if the ideal approach would be from the carotid artery, umbilical artery, or femoral vein. The fetal CMR showed clearly that the femoral vein approach with antegrade placement of the stent across the ductus was ideal. This allowed us to forego a postnatal CT and proceed directly to a catheter-based intervention at only 3 hours of life. Due to suspicion for systemic arteriopathy, genetic evaluation including chromosomal microarray and targeted gene panel testing was obtained. Whole genome sequencing identified several stretches of homozygosity (>3 Mb, comprising 5.9% of the autosomal genome); the parents are first-degree cousins. Testing for the SLC2A10 gene mutation for aortopathy came back negative.
Postnatal cardiac CT performed on day of life 7 confirmed arch continuity with supravalvar AS, a mildly hypoplastic transverse arch (4.4 mm, Z-score −2.0), severe corkscrew tortuosity of the brachiocephalic vessels, coarctation of the aortic isthmus (3.3 mm, Z-score −2.7), and an atypical posterior course of the thoracic descending aorta (Figure 8, 9, and 10). Additionally, CT demonstrated severely tortuous bilateral PA with distal tapering and hypoplasia (Figure 11), confirming the diffuse arteriopathy suspected on fetal CMR. Additional extracardiac imaging revealed extensive systemic arteriopathy on follow-up head and abdominal CT angiography with marked tortuosity of iliac, renal, carotid, vertebral, and vertebrobasilar arteries with diffusely diminutive caliber of multiple vascular territories. Following multidisciplinary discussions regarding prognosis and anticipated complexity of future interventions, the family elected to pursue comfort-focused care. As a result, planned aortic arch repair was not performed.
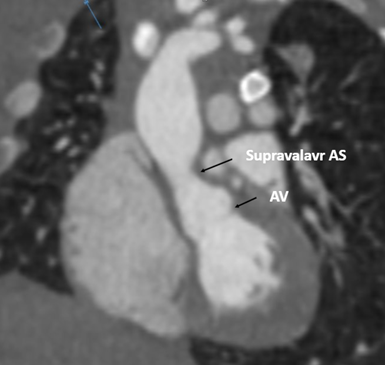 |
| Figure 8: Two-dimensional multiplanar reconstruction from postnatal cardiac CT on day of life 7, confirming supravalvar AS and a normal sized AV. |
 |
| Figure 9. Comparative multiplanar and three-dimensional rendered images of the aortic arch in the sagittal plane demonstrating arch continuity, severe corkscrew tortuosity of the brachiocephalic vessels, and an atypical posterior course of the thoracic descending aorta. |
 |
| Figure 10: Composite three-dimensional reconstruction integrating the aortic arch, bilateral PA, and PDA stent, illustrating the global vascular phenotype and the spatial relationship between systemic and pulmonary circulations following ductal stent placement. Blue color represents PA, red represents aorta, pink represents PDA stent, and brown color represents heart. |
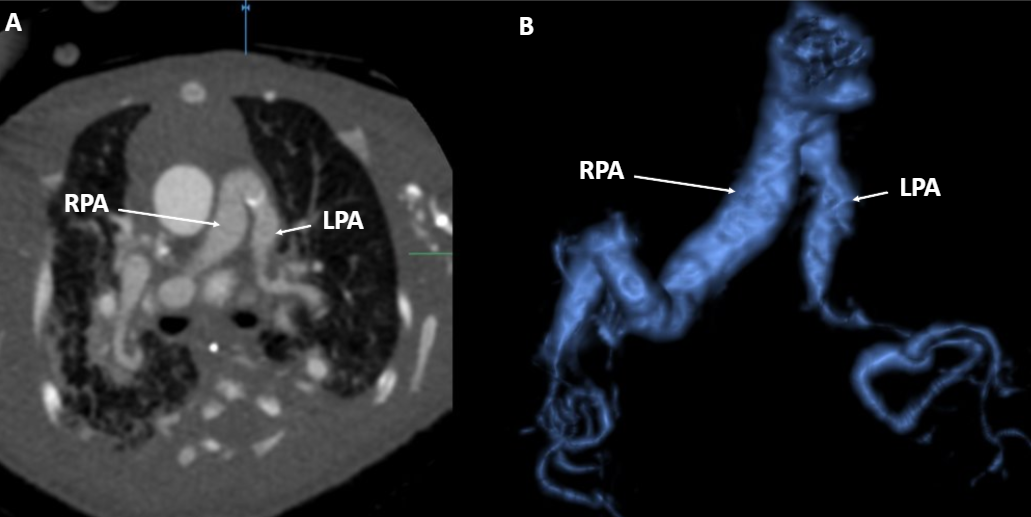 |
| Figure 11: Comparative multiplanar (A) and three-dimensional CT reconstruction (B) demonstrating severely tortuous bilateral pulmonary arteries with distal tapering and hypoplasia. Left pulmonary artery (LPA). Right pulmonary artery (RPA). |
Perspective
Historically, fetal CMR was constrained by small fetal size and motion artifact, and early consensus statements classified its role as investigational.[1] Over the past decade, Doppler ultrasound gating technology, advances in motion compensation particularly SVR and high-resolution three-dimensional isotropic reconstruction techniques have enabled its transition from a research tool to a clinically applicable modality [2-4]. Unlike fetal echocardiography, fetal CMR is not limited by fetal position, maternal body habitus, oligohydramnios, or later gestational age [5,6] In the current case, fetal CMR provided three-dimensional spatial reconstruction of the aortic arch and great vessels, delivering decisive anatomical clarifications that fetal echocardiography could not.
A key strength of this case is the high anatomical concordance between fetal CMR and postnatal cardiac CT (Figure 9). Arch continuity and tortuosity, the presence and location of supravalvar AS, RV dilation, preserved LV function, and the diffuse vascular phenotype were all accurately characterized prenatally. This level of concordance supports emerging literature demonstrating fetal CMR as a reliable clinical adjunct in complex coarctation cases and validates its role in guiding multidisciplinary perinatal planning when echocardiographic assessment is limited.[7] Suchá et al. reinforce in their 2025 comprehensive review that aortic arch and ductus arteriosus assessment represents one of the highest-yield applications of fetal cardiovascular CMR.[8] This case also illustrates the management challenge posed by the coexistence of premature ductal constriction and suspected ductal-dependent systemic circulation. Fetal CMR enabled the multidisciplinary team to anticipate this physiological conflict, provide accurate counseling, and develop a coordinated perinatal strategy. Importantly, the detailed anatomical delineation from fetal CMR directly informed planning for catheter-based intervention, allowing for rapid postnatal ductal stent placement within hours of delivery to re-establish ductal patency and effectively stabilize systemic perfusion in the presence of arch and ductal obstruction. This level of pre-procedural planning would not have been possible without precise characterization of the aortic arch and ductal anatomy.
Several limitations warrant consideration. Fetal CMR was performed at 33 weeks’ gestation, a stage at which current techniques are most effective because larger fetal size improves spatial resolution and reduces motion artifact. Consequently, fetal CMR remains primarily a late third-trimester tool, with limited applicability earlier in gestation when diagnostic clarification may have the greatest impact on counseling and pregnancy management. Image quality is also influenced by fetal position, maternal body habitus, fetal motion, and operator expertise, limiting standardization across centers. In addition, fetal CMR is resource-intensive, requiring prolonged scan times, specialized hardware, and advanced post-processing capabilities that are largely confined to experienced tertiary centers. Functional assessment remains largely qualitative, and normative fetal cardiovascular CMR reference values are not yet available.
Despite these limitations, this case demonstrates the ability of fetal CMR to accurately characterize complex cardiovascular anatomy and physiology, including the mechanism of arch obstruction and ductal restriction, facilitating targeted postnatal management. To our knowledge, this is the first reported case in which fetal CMR directly informed urgent postnatal catheter-based intervention, including ductal stenting within hours of delivery without an intervening postnatal CT examination. Although the excellent concordance between fetal CMR and postnatal findings is encouraging, conclusions are limited by the single-case nature of this report. Larger multicenter studies and registries will be necessary to establish standardized protocols, validate clinical utility, and define the role of fetal CMR in perinatal decision-making.
Click here to view the entire fetal CMR on CloudCMR.
References
- Donofrio MT, Moon-Grady AJ, Hornberger LK, et al. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation. 2014;129(21):2183-2242.
- Vollbrecht TM, Bissell MM, Kording F, et al. Fetal cardiac MRI using Doppler US gating: emerging technology and clinical implications. Radiol Cardiothorac Imaging. 2024;6(2):e230182.
- Lloyd DFA, Pushparajah K, Simpson JM, et al. Three-dimensional visualisation of the fetal heart using prenatal MRI with motion-corrected slice-volume registration: a prospective, single-centre cohort study. Lancet. 2019;393(10181):1619-1627. doi:10.1016/S0140-6736(18)32490-5
- Uus AU, Grigorescu I, van Poppel MPM, et al. Automated 3-dimensional reconstruction of the fetal thorax in the standard atlas space from motion-corrupted MRI stacks for 21-36 weeks’ gestational age range. Med Image Anal. 2022; 80:102484.
- Dong SZ, Zhu M. The role of magnetic resonance imaging in fetal congenital heart disease. Pediatr Radiol.2025;55(11):2482-2492. doi:10.1007/s00247-025-06306-2
- Cundari G, Galea N, Di Mascio D, et al. The new frontiers of fetal imaging: MRI insights into cardiovascular and thoracic structures. J Clin Med. 2024;13(16):4598. doi:10.3390/jcm13164598
- Lloyd DFA, van Poppel MPM, Pushparajah K, et al. Analysis of 3-dimensional arch anatomy, vascular flow, and postnatal outcome in cases of suspected coarctation of the aorta using fetal cardiac magnetic resonance imaging. Circ Cardiovasc Imaging. 2021;14(7):e012411. doi:10.1161/CIRCIMAGING.121.012411
- Suchá D, Bohte AE, van Ooij P, Leiner T, Schrauben EM, Grotenhuis HB. Fetal cardiovascular magnetic resonance: history, current status, and future directions. J Magn Reson Imaging. 2025;61(6):2357-2375. doi:10.1002/jmri.29664
Case prepared by:
Robert D. Tunks, MD, MHS
Editorial Board Member, Cases of SCMR
Penn State Health, Hershey, Pennsylvania USA