



Case from: Guillem Pons-Lladó, MD, FAHA; Ana-Belén Cabanillas, MR Technician
Institute: Cardiac Imaging Unit, Radiology Department, Clínica Creu Blanca Barcelona, Spain
Clinical history:
An 42 y/o asymptomatic male underwent CMR for screening of Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy (ARVD/C) as his younger brother had been recently diagnosed with ARVD/C.
CMR Findings:
SSFP cine sequences (TrueFisp) in the short-axis (Movie 1) and sagittal series (Movie 2), showed non dilated, normally contracting right and left ventricles. The longitudinal 4-chamber view (Movie 3) did not add more information on the issue. When obtaining this plane, however, a peculiar finding called the attention of the MR technician in charge of the exam: a tubular structure, apparently not artifactual in origin, appeared at the level of the atrio-ventricular plane (Figure 1, arrow). A subsequent transverse axial series of a “Black-Blood” Fast-SE sequence (Figure 2) confirmed the presence of a vessel at this level (arrows) clearly independent from an otherwise normal coronary sinus (arrowheads).
Movie 1 & Movie 2

Movie 3
The suspicion of this structure being a coronary artery of abnormal course prompted a 3D “Whole-Heart”, free-breathing, navigator-gated, non-contrast sequence oriented on crossectional views of the aortic root (Figure 3), which allowed to detect an anomalous origin of the left circumflex (LCx) coronary artery from the right coronary sinus of Valsalva, very close, but independent from the origin of the right artery (RCA). The left coronary artery (a left anterior descending, in this case) (LAD) arise from its normal origin in the left coronary sinus. The anomalous LCx is seen to course between the aortic root and the left atrium (LA) (Figure 6, arrows) on its way to the normal anatomical position of the vessel, at the left atrioventricular groove, this being the segment imaged at the 4-chamber view.
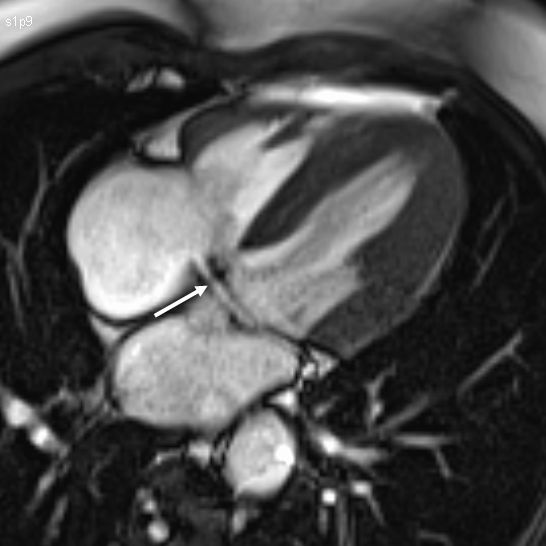
Figure 1
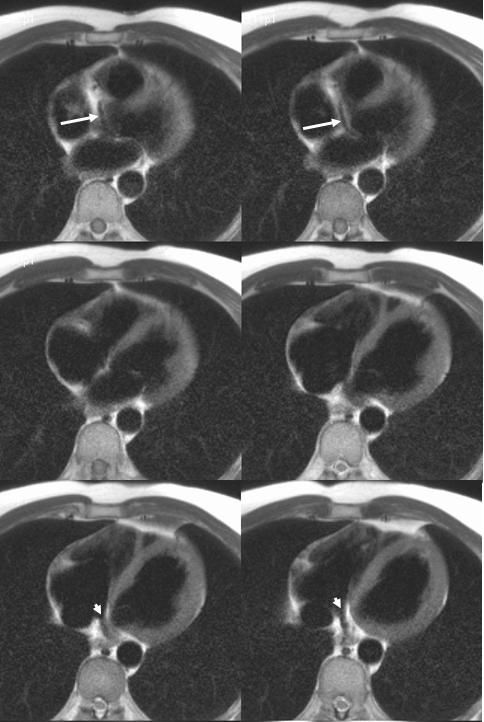
Figure 2
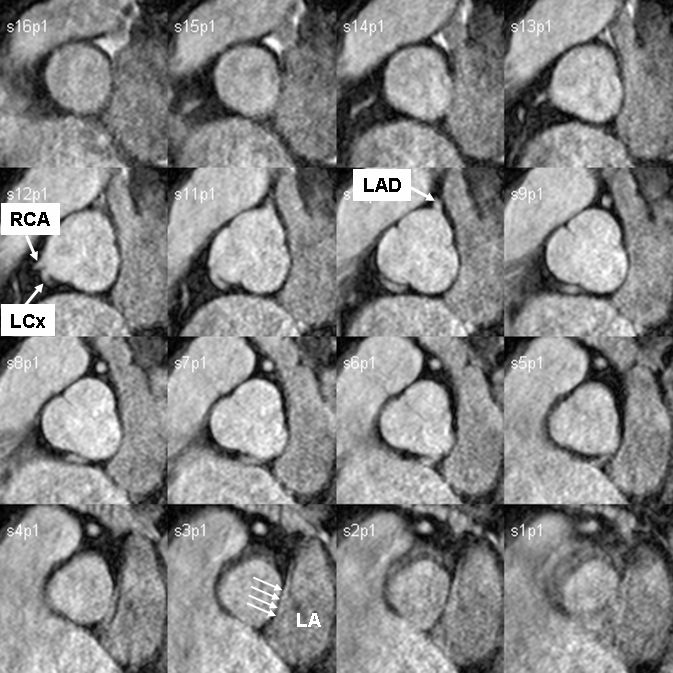
Figure 3
Conclusion: The study was reported as showing no data of ARVD/C, but with the additional finding of an anomalous origin of the LCx artery from the right coronary sinus of Valsalva and a retroaortic course. This type of congenital anomaly does not portend an adverse prognosis, and further diagnostic procedures were not recommended, provided that the patient is asymptomatic and not involved in active sport practice.
Perspective: Although Multi-Slice Computed Tomography (MSCT) compares favourably with CMR in the assessment of atherosclerotic coronary artery disease1, CMR is equally accurate in studying the origin of the vessels from the aortic root and the anatomical relationships of their proximal course, provided that the appropriate sequence is used2. As such, CMR is considered as a first line diagnostic choice in cases with a clinical suspicion of this anomaly3.
Nevertheless, the screening for the origin of the coronary arteries is not routine in a standard CMR exam, and patients with anomalous vessels may easily go undetected when studied for another condition. The alert for the presence of the anomaly came, in our case, from the detection of a definitely abnormal structure in an otherwise conventional study plane, which raised the attention of the technician, and led to a change in the study protocol.
This example highlights the relevance of the technician’s experience and attentiveness to the study acquisition, which, in the case of CMR, and in contrast to the less demanding MDCT, is essential to obtain the maximal benefit from the large amount of information that the technique is able to provide.
References:
1. Schuetz GM, Zacharopoulou NM, Schlattmann P, Dewey M. Meta-analysis: Noninvasive Coronary Angiography Using Computed Tomography Versus Magnetic Resonance Imaging. Ann Intern Med 2010; 152:167-177.
2. Prakken NH, Cramer MJ, Olimulder MA, Agostoni P, Mali WP, Velthuis BK. Screening for proximal coronary artery anomalies with 3-dimensional MR coronary angiography. Int J Cardiovasc Imaging 2010; 26: 701-710.
3. Varghese, A, Keegan, J, Pennell DJ. Cardiovascular magnetic resonance of anomalous coronary arteries. Coron Artery Dis 2005; 16: 355-364.
COTW handling editor: Vikas K. Rathi, MD, FACC
Have your say: What do you think? Latest posts on this topic from the forum

