



Institute: Univeristy Hospital of South Manchester, Manchester, UK.
Transthoracic echocardiography showed right heart dilation and severe tricuspid regurgitation with grossly abnormal, thickened and retracted tricuspid valve leaflets (Echo 1a and 1b).
A thorough review of the patient’s symptoms elicited a several years history of intermittent flushing, episodes of bronchospasm and profuse diarrhoea. She was diagnosed with carcinoid syndrome – further imaging revealed a primary pelvic tumour, but no evidence of metastatic disease and in particular no evidence of liver involvement.
A CMR scan was requested for detailed assessment of right heart involvement and the feasibility of tricuspid valve surgery.
CMR Findings: Tricuspid valve (TV) morphology was visualised by means of four chamber views, right ventricular (RV) inflow / outflow views, RV transaxial stack cine views, as well as LV short axis stack SSFP cine images.
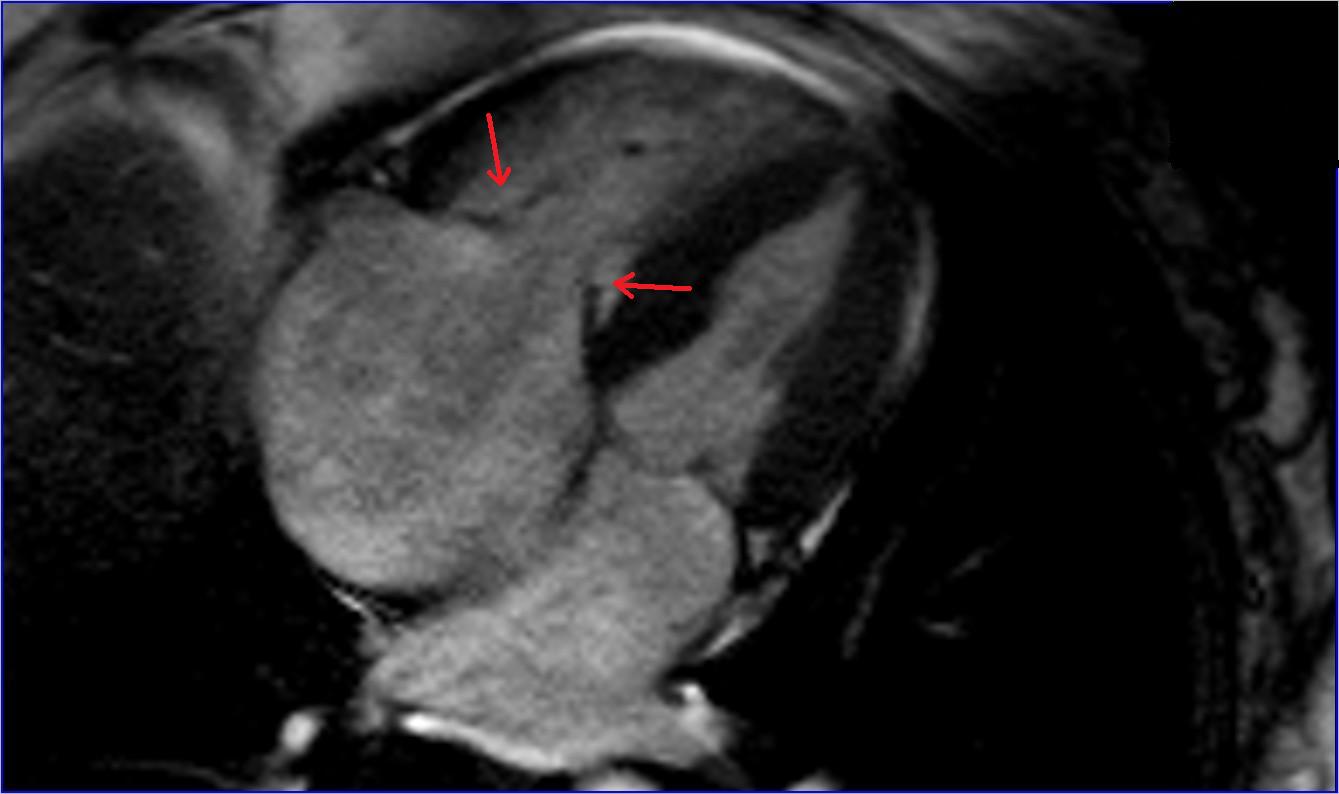
Figure 1 – End systolic SSFP frame showing the shortened and retracted septal and mural leaflet of the TV, fixed in a partially open position
The TV leaflets had typical appearance of thickening, shortening and retraction, characteristic of carcinoid TV disease. They were fixed in a partially open position throughout the cardiac cycle, with resultant severe tricuspid regurgitation (Movie 1, Fig 1, Movie 2, Movie 3, Movie 4).
Movie 1
Movie 2
Movie 3
Movie 4
An accurate calculation of RV volumes and ejection fraction was obtained from the RV transaxial stack SSFP cine views (Movie 5, Table 1). The normalized values to BSA indicate that the right ventricular volumes are mildly elevated.
Movie 5
Right ventricular trans-axial stack
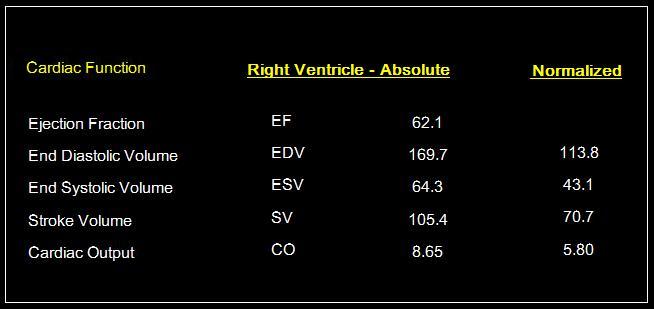
Table 1 – Volumetric measurements for the Right Ventricle – Values normalized to BSA
There was interventricular septal flattening with typical D-shaped left ventricle (LV) in diastole seen in the short axis LV SSFP cine stack views suggestive of RV volume overload (Movie 6).

Movie 6
SSFP – RV & LV short axis cine
Movie 7a
Movie 7b
The tricuspid regurgitation (TR) was quantified by the TR regurgitant volume, derived using the indirect method of subtracting the pulmonary forward flow (54 mls) from the right ventricular stroke volume (RV SV = 105 mls). This gave an estimated regurgitation volume of 51 mls and a regurgitation fraction of 49%, in keeping with severe TR. The pulmonary forward flow was estimated using through plane phase contrast velocity mapping positioned just above the level of the pulmonary valve whilst the RV SV was estimated by contouring volumes of the RV transaxial stacks in systole and diastole.
We further quantified the tricuspid regurgitation via through-plane flow mapping at the level of the tricuspid valve (Movie 7a and 7b). This is usually a less precise method, limited by difficulties in outlining accurately the tricuspid valve orifice as a consequence of significant through plane motion that occurs at this level throughout the cardiac cycle. However, in the presented pathology, the TV orifice area was rather fixed. This situation allowed this method of quantification to be applied with a higher dergee of accuracy, as evidenced by the obtained regurgitant fraction of 46%, consistent with the indirect volumetric method result (Fig 2).
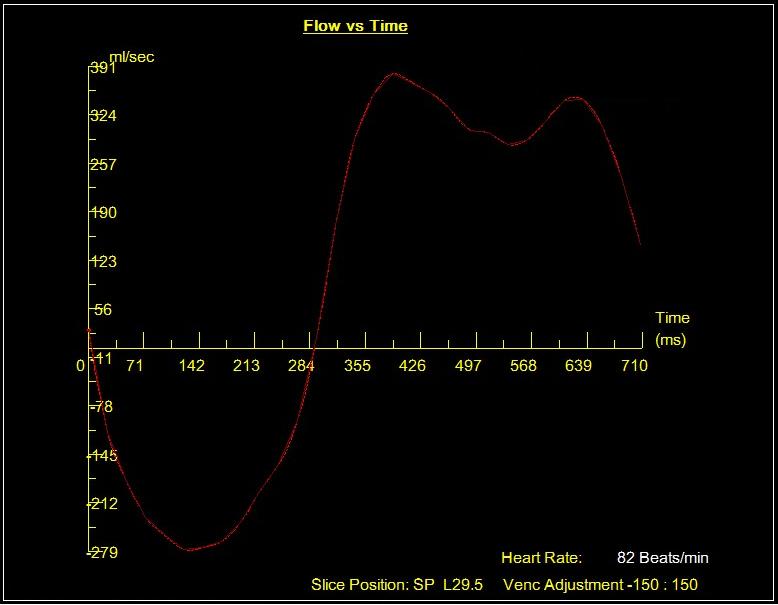
Figure 2
Sagittal views of the IVC and its drainage into the RA were obtained (Movie 8), with in-plane and through-plane velocity mapping of the RA inflow at the level of the proximal IVC for detection and quantification of venous flow reversal related to the severe tricuspid regurgitation.
Movie 8
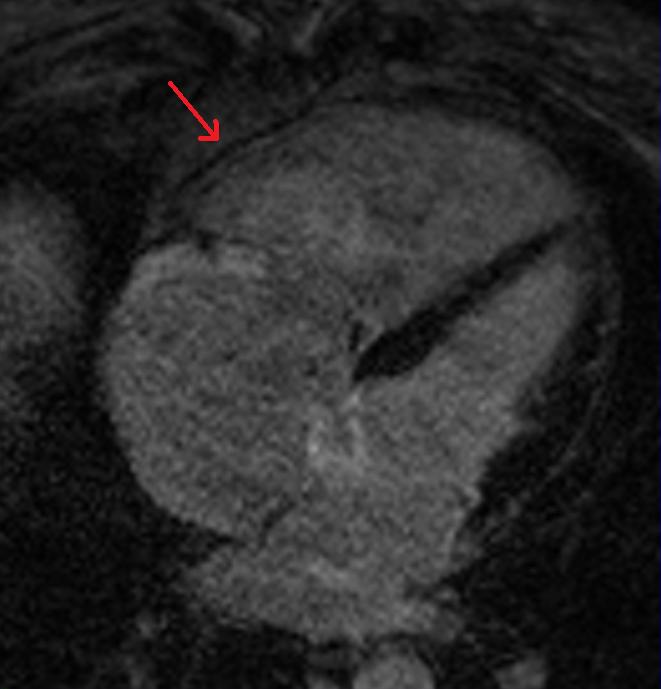
Figure 3a
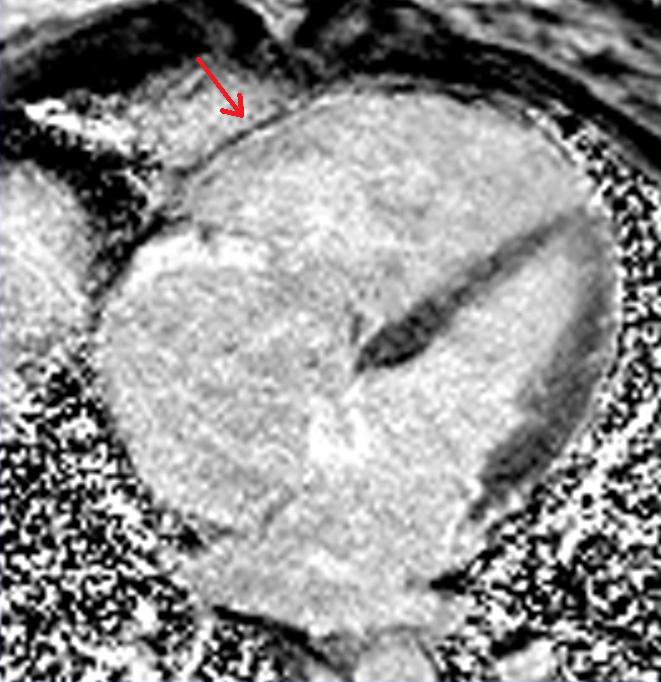
Figure 3b
Late gadolinium enchancement T1 inversion recovery and phase sensitive inversion recovery imaging was performed to look for hyperenhancement within the RV wall (Fig 3a and 3b, Fig 4a and 4b). Although there was no evidence of obvious late gadolinium uptake, there appeared to be thinning of the RV free wall with the appearance of chemical shift artefact at the myocardium – blood pool interface. There was no evidence of intracardiac metastatic disease. Of note, there is late gadolinium enhancement of the anterior tricuspid valve leaflet.
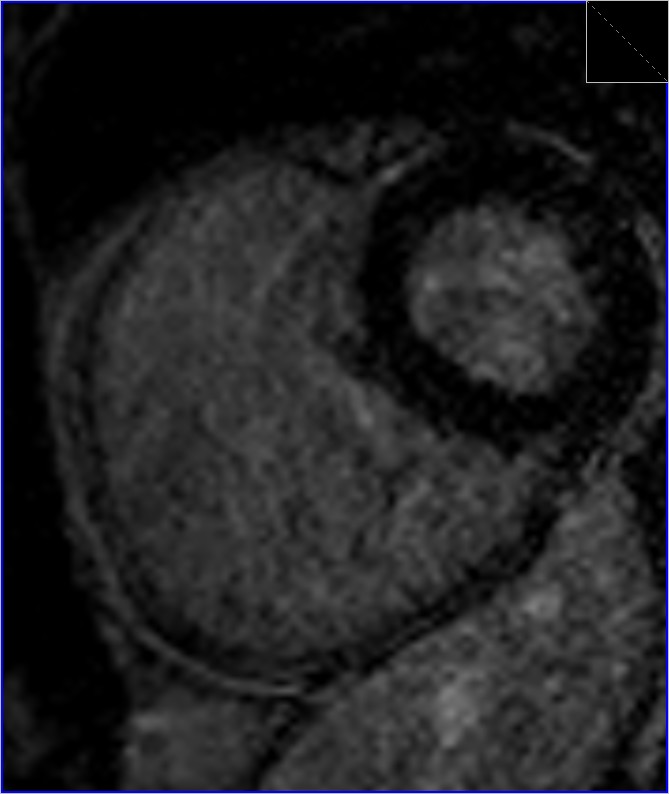
Figure 4a

Figure 4b
Conclusion: This study illustrates a typical case of right heart valve involvement in carcinoid syndrome with evidence of RV volume loading, dilation and thinning of the RV free wall. The preserved RV systolic function is a favourable prognostic factor for patients who are being worked up for valve replacement surgery.
The fixed nature of the fibrosed tricuspid valve leaflets facilitates quantification of tricuspid regurgitation by the through-plane flow mapping method, which would usually be inprecise in cases where the tricuspid valve has preserved excursion at annular and leaflet level.
The presence of cardiac involvement in carcinoid syndrome imparts a dramatic deterioration in prognosis with a 50% increase in mortality. There is evidence that surgical correction of the valve abnormalities not only improves symptoms but also overall prognosis and thus should be considered in appropriately selected patients [3,4].
CMR evaluation of RV function and volumes, as well as accurate calculation of valvular regurgitant fractions, is helpful for a more detailed pre-operative assessment and patient risk stratification [5].
References:
1. Fox DJ, Khattar RS. Carcinoid heart disease: presentation, diagnosis, and management, Heart. 2004; 90(10):1224-1228
2. Bernheim AM, Connolly HM, Hobday TJ, Abel MD, Pellikka PA. Carcinoid Heart Disease, Progress in Cardiovascular Diseases. 2007; 49(6):439-451
3. Connolly HM, Nishimura RA, Smith HC, Pellikka PA, Mullany CJ, Kvols LK. Outcome of cardiac surgery for carcinoid heart disease, J Am Coll Cardiol. 1995; 25(2):410-6.
4.Castillo JG, Filsoufi F, Rahmanian PB, Anyanwu A, Zacks JS, Warner RR, Adams DH. Early and late results of valvular surgery for carcinoid heart disease, J Am Coll Cardiol. 2008; 51(15): 1507-9
5. Sandmann H, Pakkal M, Steeds R. Cardiovascular magnetic resonance imaging in the assessment of carcinoid heart disease Clin Radiol. 2009; 64(8):761-6
Submit your case here
COTW handling editor: Monica Deac

