



Case from: Baskar Sekar, Michael D Sosin, Thomas P Mathew
Institute: Trent Cardiac Centre, Nottingham University Hospital – city campus, Nottingham, United Kingdom
Background: Primary cardiac neoplasms are rare with an incidence of ~0.02%1. Most malignant cardiac tumours are sarcomas2 and they usually involve right atrium3. They can be mistaken for myxomas especially when they are present in the left atrium. Diagnosis is often not made pre-operatively or antemortem. Though echocardiography is an useful initial investigation, cardiac MRI (CMR) is the most effective technique for tissue identification and staging.
Clinical History: A previously well 53-year-old man presented with a 3 week history of breathlessness. Clinical examination revealed an irregularly irregular pulse and a pan-systolic murmur. Transthoracic Echocardiography (TTE) showed a large mass filling the left atrium (4.0 x 6.0cm) and prolapsing through the mitral valve (Figure 1, Video 1).
Video 1: TTE of left atrial (LA) mass

Video 1: TTE of left atrial (LA) mass
Cardiac MRI: Cardiac gated steady-state free precession (SSFP) sequence during CMR showed two distinct masses with low signal intensity, one arising from the right lower pulmonary vein and the second attached with a broad base to the interatrial septum (Figure 2, Video 2). This appearance excluded a myxoma.

Video 2: Cine SSFP LA mass
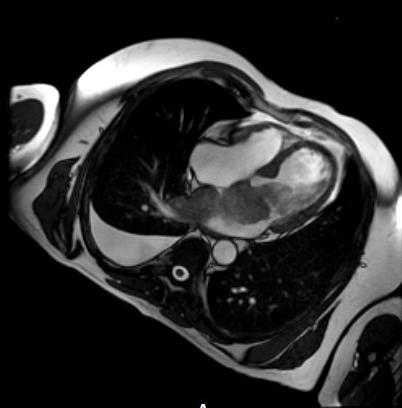
Figure 2: SSFP LA mass
The mass was similar in signal intensity to myocardium on T1 weighted spin echo (Figure 3) and had a high signal intensity on T2 weighted images with the brightness persisting on fat saturated images (Figure 4) excluding a lipoma or liposarcoma. There was minimal contrast uptake during first pass perfusion (excluding angiosarcoma) with generalised uptake of contrast with an irregular border on late gadolinium enhanced images (Figure 5).

Figure 3: T1-weighted spin echo
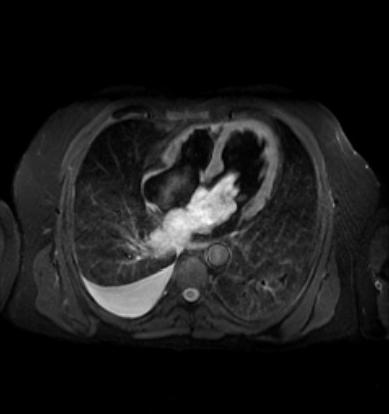
Figure 4: T2-weighted fat saturated spin echo

Figure 5: PSIR delayed enhancement
At surgery the tumour was extensively debulked but complete removal was not possible. Histopathology confirmed high grade primary sarcoma (Figure 6).
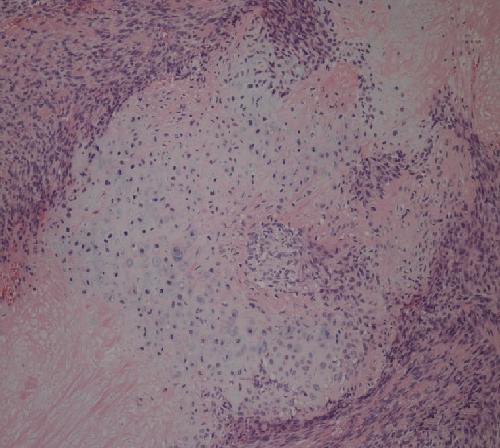
Figure 6: Microscopy of LA sarcoma
Perspective: Primary cardiac sarcomas are extremely rare and are often difficult to differentiate from a myxoma when the tumour is confined to the left atrium. This case illustrates the role of multimodality imaging and the strengths of CMR to delineate the extent and relationship of the tumour to other cardiac structures and the various sequences that can be used for tissue characterisation.
References:
1. Sarjeant JM, Butany J, Cusimano RJ. Cancer of heart: epidemiology and management of primary tumors and metastases. Am J Cardiovasc Drugs 2003;3:407-421.
2. Burke AP, Cowan D, Virmani R. Primary cardiac sarcoma of the heart. Cancer 1992;69:387-395.
3. Khadilkar UN, Harish R, Tantry G, Kumar S, Tiwari A. Primary cardiac sarcoma. Indian J Pathol Microbiol. 2008 Jan-Mar;51(1):30-31.
COTW handling editor: Kevin Steel

