



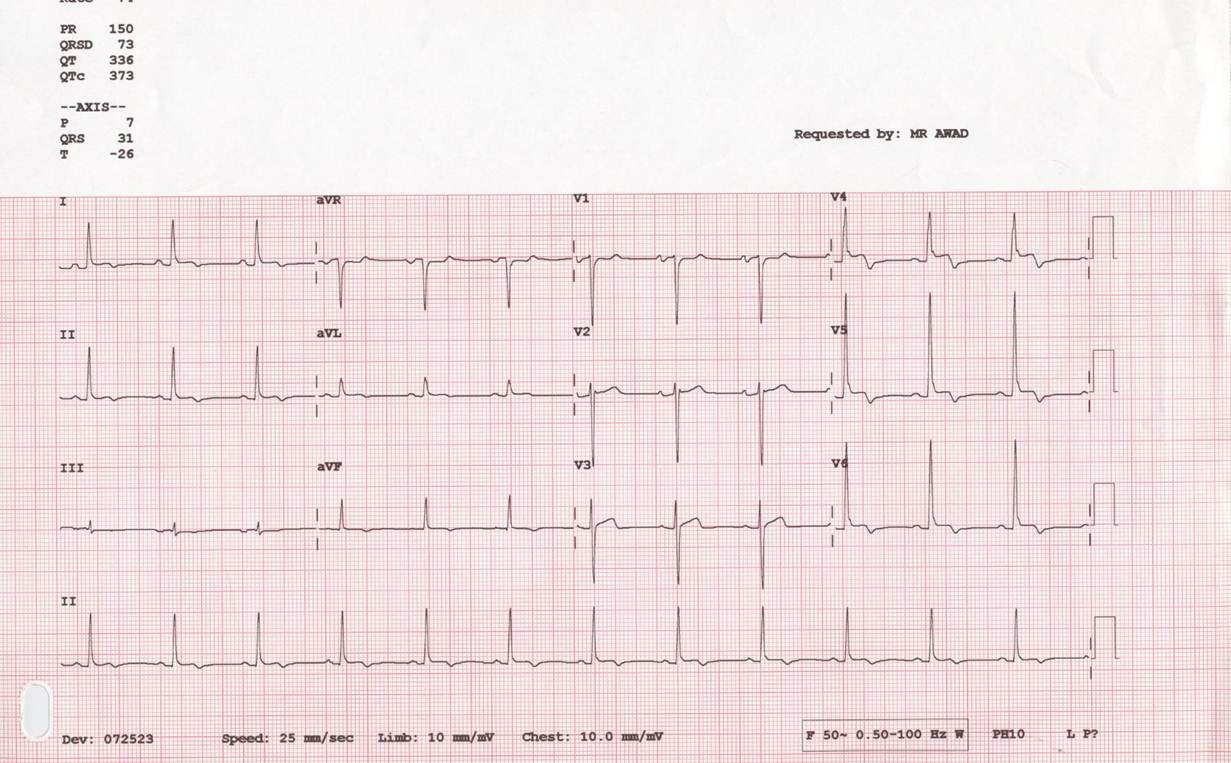
Figure 1: ECG with nonspecific T wave changes
Transthoracic echocardiogram (TTE) showed a large right atrial mass associated with the right atrial free wall, small pericardial effusion, normal valves and preserved systolic function (Movies 1-4). The differential diagnosis included atrial thrombus, myxoma or primary or secondary cardiac tumour.
Movie 1: TTE (PLAX) with pericardial effusion & Movie 2: TTE (SAX) with pericardial effusion
Movie 3: TTE (SAX) with right atrial mass & Movie 4: TTE (Apical) with right atrial mass

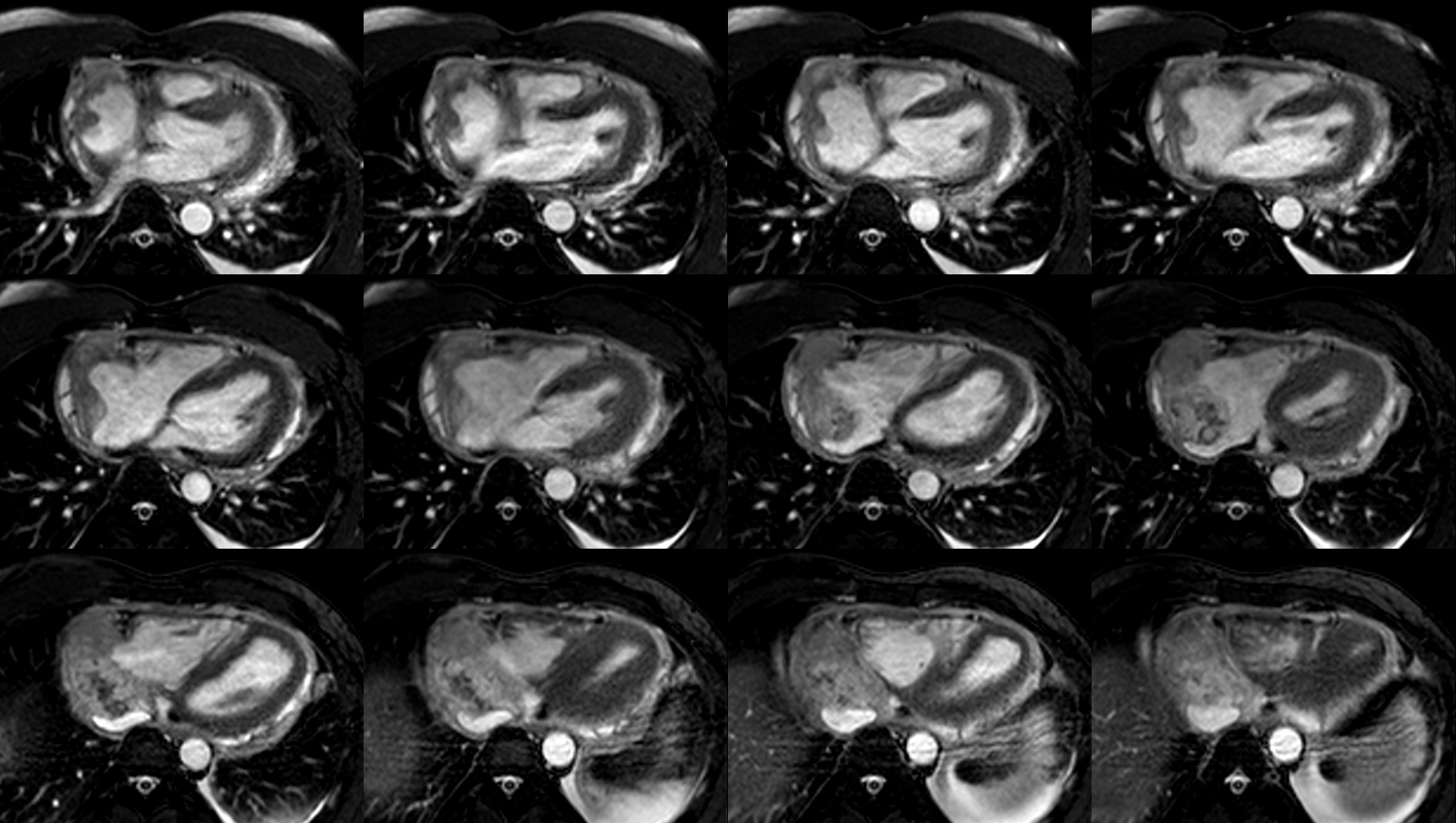
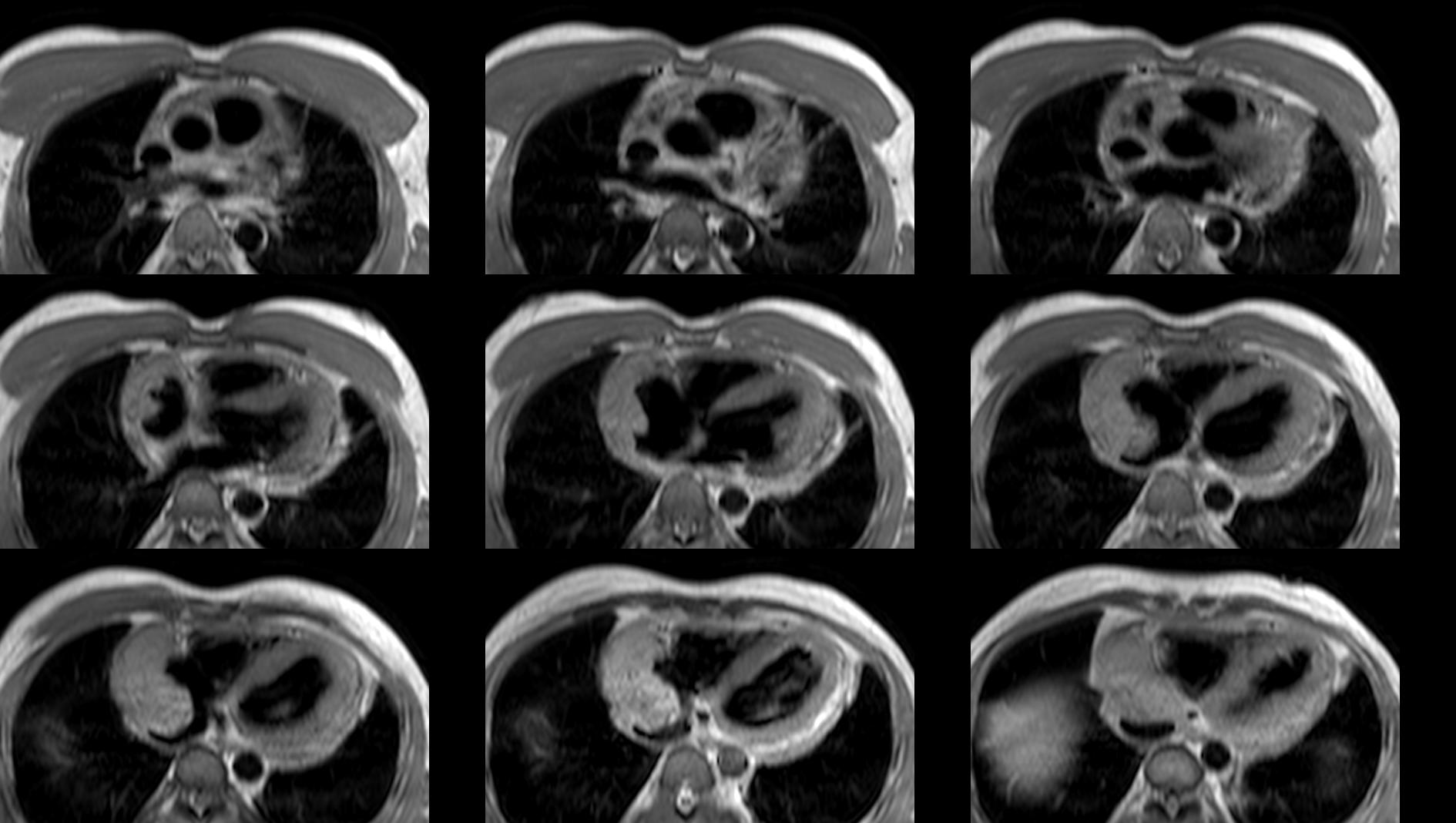
Figure 2: Axial SSFP & Figure 3: Axial black-blood
T2-STIR imaging showed areas of increased signal intensity within the RA mass suggesting oedema (Fig 4). There was no fatty infiltration of the mass (Fig 5).
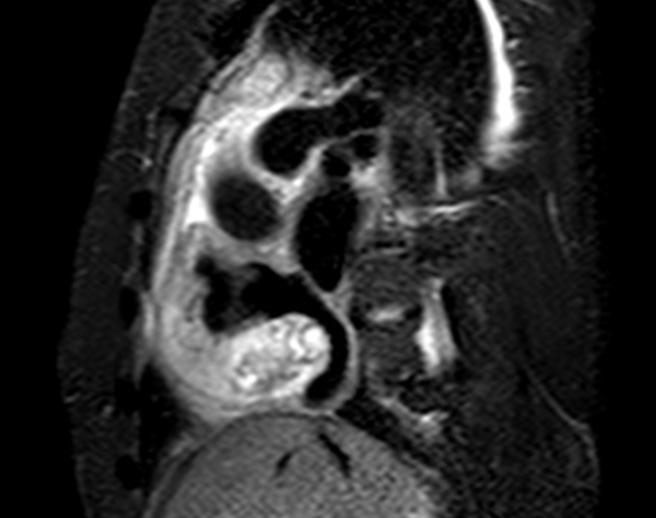
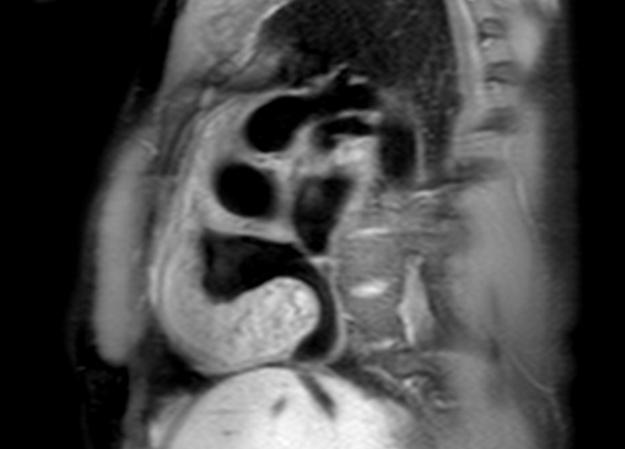
Figure 4: T2-STIR & Figure 5: Fat-sat black blood
Rest perfusion showed a large avascular area that would be consistent with areas of necrosis (Movie 6).

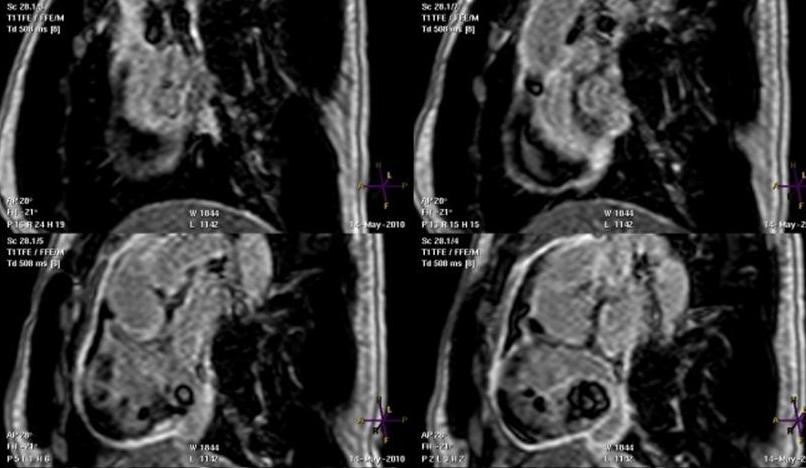
Figure 7: Early enhancement & Figure 8: Late enhancement
Follow up: The patient underwent attempted excision of the mass. However, at surgical exploration through median sternotomy, the mass was clearly too extensive for surgical excision. There were multiple masses present within the pericardium with extensive adhesions. The major mass was occupying the right atrium and felt solid. The SVC felt hard on palpation, however, there was no direct obstruction of SVC or IVC. There was a further separate mass overlying the aorta and pulmonary artery anteriorly. Multiple biopsies were taken for further examination.
The histology of the specimens showed fibroconnective tissue invaded by a malignant tumour. The tumour was composed of small dark epithelioid cells arranged in solid sheets and cords with limited eosinophilic cytoplasm and focal vasoformative arrangement. Frequent mitotic figures were present. The stroma was fibrotic and showed chronic inflammation and haemosiderophages. The microscopic and immunohistochemical profile were consistent with an angiosarcoma.
Perspective: Angiosarcomas are the most common primary malignant neoplasm of the heart. The incidence peaks in the third to fifth decade and are more common in males. Ninety percent of the angiosarcomas are located in the right atrium. The most common site being the free wall and the septum being spared in most cases.
A variety of imaging modalities are available in the work up of a patient with a cardiac mass. Cardiac MRI enables the most comprehensive imaging assessment of cardiac masses. In contrast to other modalities, MRI provides improved soft tissue contrast, tissue characterisation as well as assessment of mediastinal and lung involvement by the tumour. Additional imaging with gadolinium contrast allows further characterisation of the tissue, the extent of vascular supply and further improves the differentiation from surrounding tissue.
The treatment of angiosarcomas are dictated by the local extent of the tumour and metastatic spread. Surgical resection or debulking of the tumour is indicated where possible. Additional treatment with chemotherapy, irradiation and cardiac transplantation have been reported with no significant impact on survival.
References:
- Burke A, Jeudy J, Virmani R. Cardiac tumours: an update. Heart 2008 94: 117-123.
- Randhawa K, Ganeshan A, Hoey E. Magnetic resonance imaging of cardiac tumours: Part 2, Malignant tumours and tumour like conditions. Curr Probl Diagn Radiol 2011 July/August: 169-179.
COTW handling editor: Kevin Steel
Have your say: What do you think? Latest posts on this topic from the forum