



Arun Dahiya1,3, Lamia Jamjoom2, Wael Aljaroudi1 , Rahul Renapurkar2 , Michael Bolen2
Institute: 1Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio , 2Imaging Institute, Cleveland Clinic, Cleveland, Ohio, 3Royal Brisbane Hospital, Brisbane, Australia
Clinical history: A 59 year old female two months post abdominal hysterectomy, bilateral salpingo-oophorectomy for a high grade endometrial leimyosarcoma, underwent a staging chest CT scan at an outside hospital that revealed a possible cardiac mass in the left atrium. Subsequent transthoracic echocardiography although identified the mass, was unable to adequately define the extent of this left atrial mass (Video 1). Patient was referred to our institution for cardiac MRI to further define the extent and characterize this finding.
CMR Findings: Cine SSFP images (Video 2,3,4) revealed a left atrial mass with broad based attachment. In addition there was a low signal intensity mass noted in the left pulmonary artery which was mobile in SSPF cine imaging [Video3,4 (Small arrow)]. LA mass appeared iso-intense on T1-W images (Fig 1- Large arrow) and hyper-intense on edema weighted imaging (Fig 2- arrow) and perfusion imaging confirmed brisk vascularity with a central necrotic core, while the mobile left pulmonary artery mass failed to enhance on perfusion imaging(Video 4). Post gadolinium enhancement imaging (Fig 4) revealed enhancement in the area of necrotic core (Large arrow). These findings were most consistent with a metastatic left atrial tumor and an incidentally discovered pulmonary embolus. Patient was admitted to the hospital for anticoagulation. Unfortunately patient was deemed inoperable and managed with chemotherapy with regular surveillance by CMR.

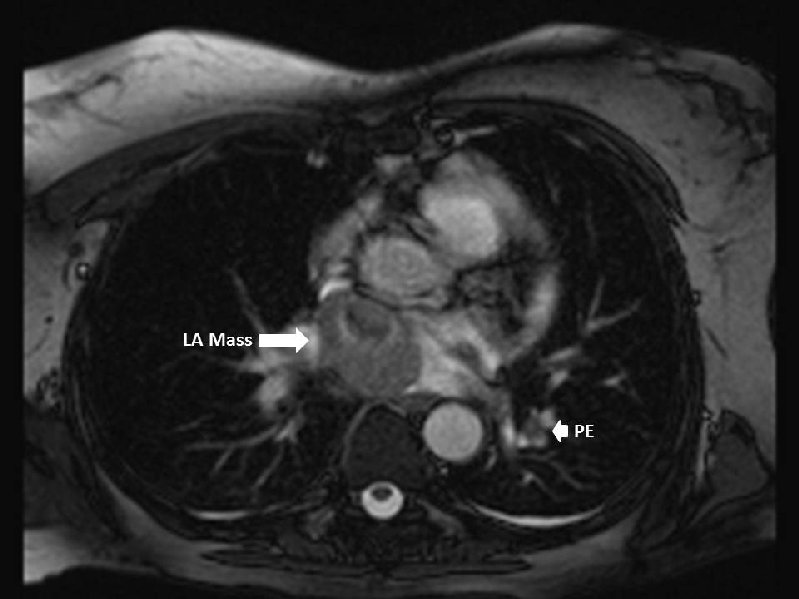
Fig 1
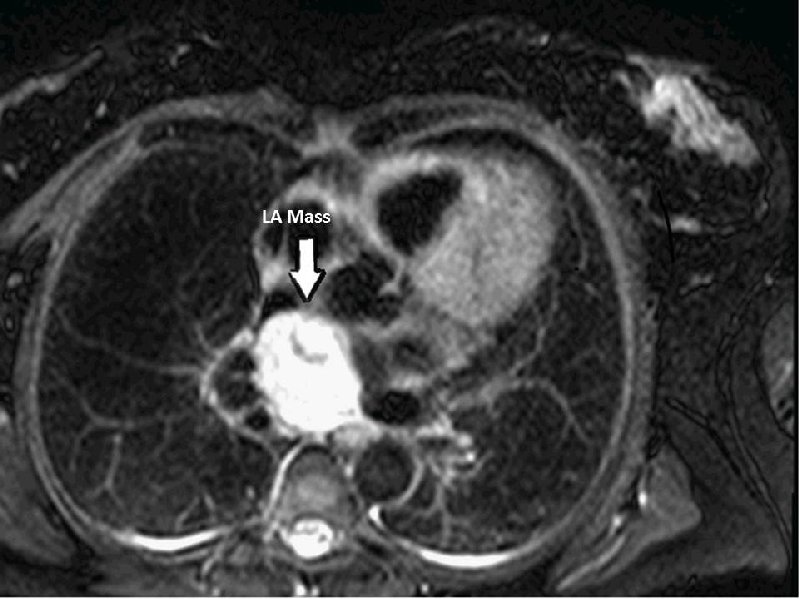

Fig 2 & Fig 3
Discussion: Cardiac masses are frequently encountered in clinical practice and in absence of obvious thrombus predisposing echocardiographic features (eg. regional wall motion abnormalities, catheters, atrial fibrillation etc) are given differential diagnoses of a cardiac tumor. The frequency of cardiac tumors vary from 0.1% to 0.3% in most autopsy series (1).
Benign tumors make 75% of all cardiac tumors (myxoma 52%, papillary fibroelastomas 16% , lipoma 16% and hemangioma 6% (1). Remaining 25% of cardiac tumors are malignant and are predominately made up by secondary tumors or directly invading tumors with primary malignant tumors being rare(sarcoma 5% and lymphoma 9%) (2). As these tumors can lead to adverse outcomes ranging from local mechanical complications to thromboembolism they warrant prompt evaluation and management. For these reasons initial diagnoses of suspected cardiac tumor can cause significant patient and clinician anxiety and triggers further supplementary imaging by cardiac MRI. Cardiac MRI can not only define the extent, invasive nature of the mass but also provide additional insights into pathology of the mass by tissue characterization (3). However CMR evaluation of cardiac masses should not only evaluate the cardiac mass but should also include comprehensive assessment of cardiac function as well as screening for any incidental finding such as pulmonary embolism. In a metanalysis of more than 10000 patients undergoing CT scan for reasons other than suspected PE, prevalence of pulmonary embolism was estimated to be 2.6% (4). In this analysis Hospitalization at the time of CT scanning and the presence of cancer were associated with a significantly increased risk of incidental PE (4).
Perspective: CMR is increasingly used for evaluating cardiac masses. This report not only demonstrates incremental value of CMR in the assessment of cardiac masses but also highlights the importance careful comprehensive assessment of secondary findings in a patient with suspected cardiac malignancy.
References:
1. Roberts WC. Primary and secondary neoplasms of the heart. Am J Cardiol 1997;80:671-682.
2. Altbach MI, Squire SW, Kudithipudi V, Castellano L, Sorrell VL. Cardiac MRI is complementary to echocardiography in the assessment of cardiac masses. Echocardiography 2007;24:286-300.
3. Beroukhim RS, Prakash A, Buechel ER, Cava JR, Dorfman AL, Festa P, Hlavacek AM, Johnson TR, Keller MS, Krishnamurthy R, Misra N, Moniotte S, Parks WJ, Powell AJ, Soriano BD, Srichai MB, Yoo SJ, Zhou J, Geva T. Characterization of cardiac tumors in children by cardiovascular magnetic resonance imaging: a multicenter experience. J Am Coll Cardiol 2011;58:1044-1054.
4. Dentali F, Ageno W, Becattini C, Galli L, Gianni M, Riva N, Imberti D, Squizzato A, Venco A, Agnelli G. Prevalence and clinical history of incidental, asymptomatic pulmonary embolism: a meta-analysis. Thromb Res 2010;125:518-522.
COTW handling editor: Vikas K. Rathi, MD, FACC
Have your say: What do you think? Latest posts on this topic from the forum