



Case from: Víctor Pineda MD1, Sarai Roche MD1, Hug Cuellar MD1, Teresa González-Alujas MD2
Institute: 1. Hospital Universitari Vall d’Hebron. Radiology Departament (Barcelona/Spain)
2. Hospital Universitari Vall d´Hebron. Cardiology Departament (Barcelona/ Spain)
Clinical history: A 60-year-old man, originally from Sardinia, with diabetes and hypertension presented with sporadic, nonspecific precordial discomfort of short duration. The ECG showed sinus rhythm and a very broad right bundle branch block. Frontal and lateral radiographs depicted cardiomegaly with alteration of the cardiac silhouette due to the presence of a round, peripherally calcified lesion (arrows) located in the superolateral portion of the left ventricle (fig.1). A multidetector gated cardiac CT demonstrated a large, round, perfectly delineated homogeneous lesion surrounded by a linear “egg-shell” calcification (arrows). The lesion had a mass effect in the left coronary tree, without compression of the coronary arteries (fig. 2).
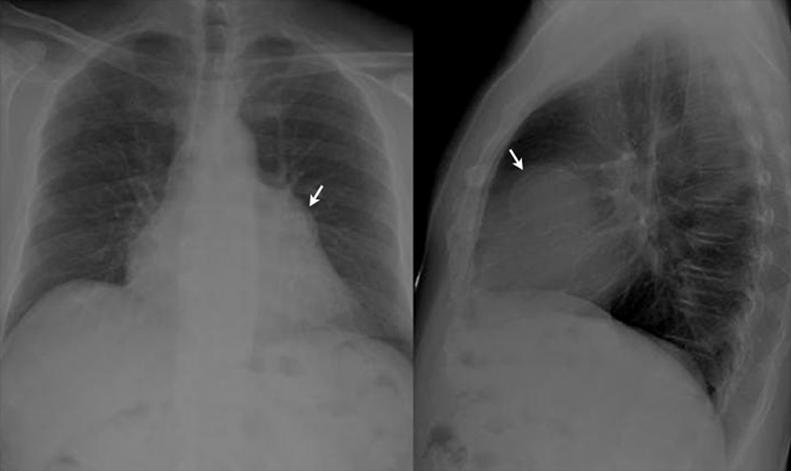
Figure 1: Frontal and lateral radiographs shows an alteration of the cardiac silhouette due to the
peripherally calcified lesion (arrows)
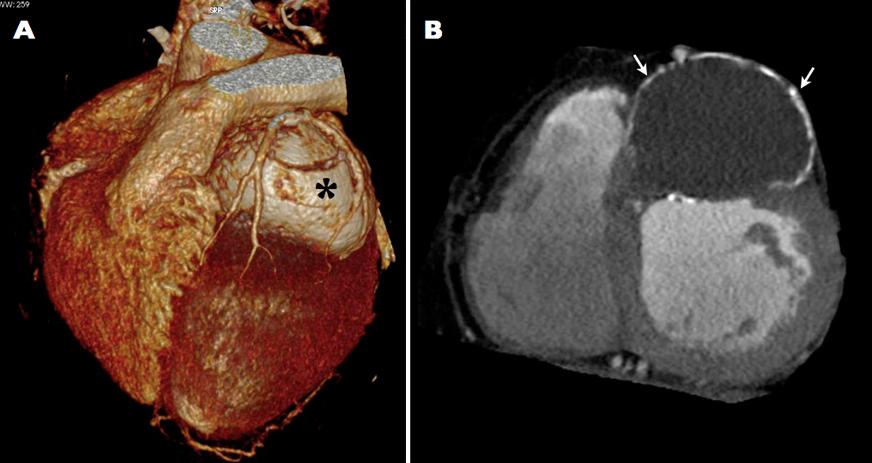
Figure 2: A) 3D volume rendered cardiac CT and B) short-axis reformation of contrast-enhanced cardiac CT scan shows large left ventricular lesion (asterisk) surrounded by a linear calcification (arrows) with mass effect in the left coronary tree
CMR Findings: On magnetic resonance imaging, steady state free precession short-axis cine-MRI demonstrated a large well-defined mass within the LV anterior wall (movie 1). Turbo spin echo T2-weighted MR imaging showed an intramyocardial cystic lesion with a hypointense capsule and an internal laminated appearance (fig. 3A). Delayed contrast-enhanced imaging depicted intense peripheral capsular enhancement related to pericystic fibrous changes (fig. 3B).

Movie 1: Steady state free precession short-axis cine loop
demonstrates a large well-defined mass within the LV anterior wall
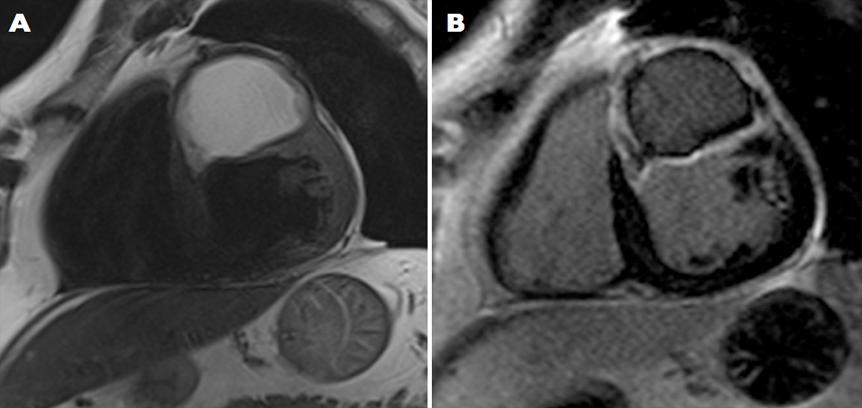
Figure 3: A) short-axis TSE T2-weighted imaging shows an intramyocardial cystic lesion with a hypointense laminated capsule and B) short-axis delayed contrast-enhanced cardiac MR imaging demonstrating intense peripheral capsular enhancement related to pericystic fibrous reactive myocardial tissue
Conclusion: The case presented had several radiologic findings that suggested the specific diagnosis of hydatid cyst: 1) peripheral calcification that was clearly visible on MDCT images, 2) internal membrane detachment, and 3) a hypointense external fibrous layer on T2-weighted MR sequences that markedly enhanced on delayed contrast-enhanced images related to pericystic fibrous reactive myocardial tissue. The serological tests confirmed the diagnosis of cardiac hydatid disease.
Perspective: Hydatid cyst, which is produced by the larvae of the parasite, Echinococcus granulosus, most commonly affects the liver or lungs. Cardiac involvement is uncommon and accounts for only 0.5%-2% of cases. Symptoms may be absent or non-specific, and include chest pain, dyspnea on exertion, palpitations, fever, or conduction alterations. The most serious potential complication is cyst rupture, which can trigger anaphylactic shock, cardiac tamponade, or pulmonary or systemic embolization (1). In this particular case, the patient experienced chest pain as well as a right bundle branch block. This electrocardiographic finding may be due to compression on the right bundle from the cyst itself.
Histologically, hydatid cyst consists of three layers: the protective outer layer or pericyst, formed principally by fibrous reactive tissue of the host; the middle layer of permeable laminated membrane; and the inner or germinal layer (2-3).
MRI can adequately characterize the cystic nature of the lesion, with the typical hypointense ring of the wall and internal laminated appearance (4). The peripheral ring corresponds to the pericyst, comprised of fibrous reactive myocardial tissue. In the case presented, the pericyst could be clearly seen on delayed contrast-enhanced cardiac MR imaging, which showed intense peripheral enhancement of the lesion. To the best of our knowledge, this is the first description of pericystic fibrous reactive myocardial tissue depicted by delayed contrast-enhanced cardiac MR imaging.
References:
1. Dighiero J, Canabal EJ. Echinococcus disease of the heart. Circulation 1958; 17: 127-132.
2. Beggs I. The radiology of hydatid disease. Am J Roentgenol. 1985; 145:639-648.
3. Lewall DB. Hydatid disease: biology, pathology, imaging and classification. Clin Radiol 1998; 52:863-874.
4. Dursun M, Terzibasioglu E, Yilmaz R, Cekrezi B, Olgar S, Nisli K, Tunaci A. Cardiac hydatid disease: CT and MRI findings. Am J Roentgenol. 2008;190(1):226-32.
COTW handling editor: Kevin Steel
Have your say: What do you think? Latest posts on this topic from the forum