



Case from:
Masoud Shariat, MD1, Lars Grosse-Wortmann, MD1, 2, Shi-Joon Yoo, MD1
Institute:
1 Department of Diagnostic Imaging, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada
2Labatt Family Heart Centre at The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada
Clinical history:
An asymptomatic fifteen-year-old boy with dextrocardia and complete transposition of the great arteries (CTGA) who had arterial switch operation and closure of ventricular septal defect (VSD) during infancy was referred for baseline Cardiac Magnetic Resonance (CMR) study.
CMR findings:
In addition to typical findings in a complete transposition of great arteries after arterial switch operation, including the pulmonary artery bifurcation anterior to the ascending aorta, as well as dextrocardia, CMR images demonstrated the atrioventricular (AV) valves to be located at different planes with non-parallel opening axes (movie 1, figure 1 and figure 2).


Movie 1 and Figure 1: Cine SSFP in two-chamber orientation of the left ventricle. The left atrioventricular valve is seen in profile and the opening of the right AV valve is en face. Figure 1 is a still frame of the same orientation with labels on the right atrioventricular valve (RAVV) and left atrioventricular valve (LAVV).
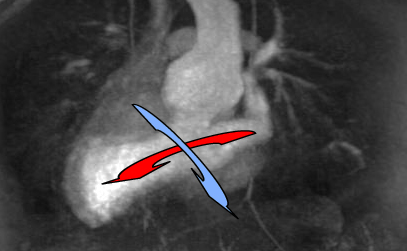
Figure 2: Non-parallel opening axes of atrioventricular valves. Red arrow: left atrioventricular axis. Blue arrow: right atrioventricular axis.
The right AV connection had a postero-anterior orientation and the left AV connection was oriented from left to right (figures 3a and 3b).
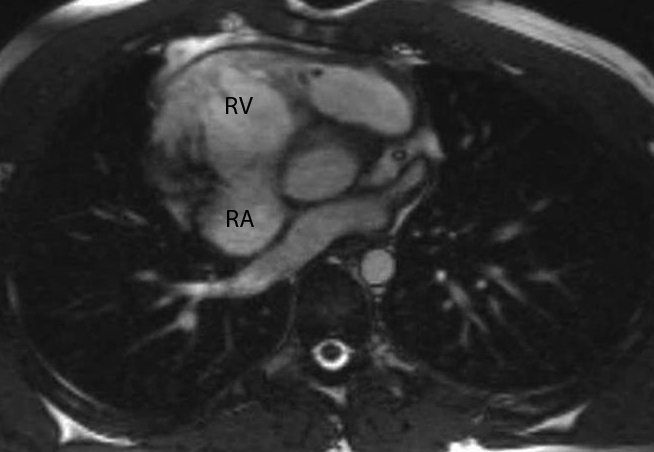
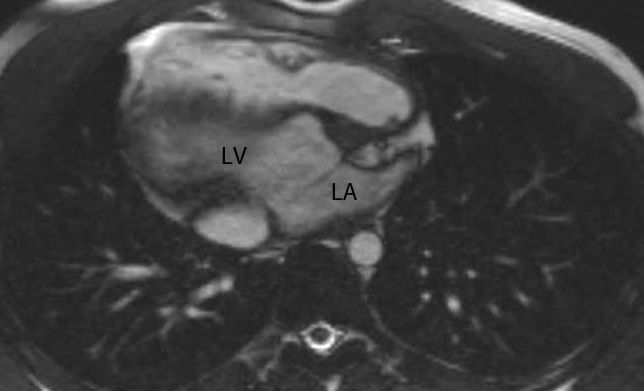
Figures 3a and 3b: Right atrioventricular connection has postero-anterior orientation while left atrioventricular connection is oriented from left to right. RA: right atrium, RV: right ventricle, LA: left atrium, LV: left ventricle
The right ventricle was located antero-superiorly and left ventricle was postero-inferiorly located. The right atrium was elongated and stretched cranially to connect to the superiorly located right ventricle (figures 4a and 4b).
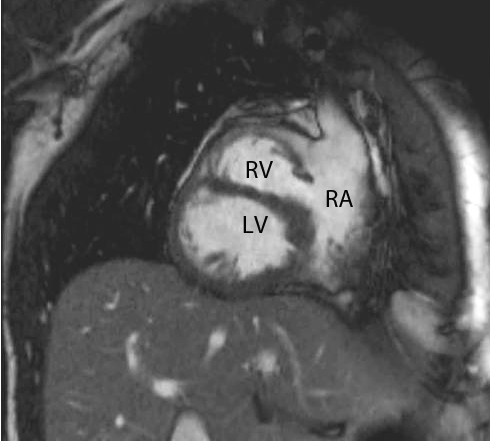
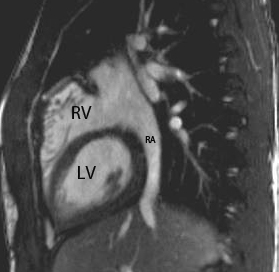
Figures 4a and 4b: Elongated right atrium in direct contact with the left ventricle. RA: right atrium, RV: right ventricle, LV: left ventricle
A good overview of the anatomy is shown in a stack of axial cine steady state free precession (SSFP) images (Movie 2).
Movie 2: Axial cine SSFP stack showing a good overview of the anatomy
Based on these findings the diagnosis of twisted atrioventricular connection or criss-cross heart was made in this patient.
Twisted atrioventricular connection or criss-cross heart is a condition in which AV valves have non-parallel opening axes of AV valves. As a result of this anatomy, the apex of each ventricle is located on the opposite side of the atrium it is connected to, there is elongation of the right atrium with the tricuspid valve in this case located high in the right atrium and the left ventricle is usually in direct contact with right atrium. All these features can be clearly appreciated on CMR (1)
Discussion:
This was an unexpected diagnosis of twisted atrioventricular connection in a patient with repaired CTGA and VSD. Twisted atrioventricular connection or criss-cross heart is a rare congenital cardiac abnormality. Its frequency is less than eight per 1, 000,000 accounting for less than 0.1% of congenital heart anomalies (2). Twisted atrioventricular connections are caused by a loss of normal parallel axes of ventricular inlets, ranging from mild twisting of the ventricles to an overt criss-crossed relationship in extreme cases. Other features of this pathology include atrial septum angulation, curved ventricular septum, and unusual relationships of the great arteries for a given pathology (3).
Perspective:
Twisted atrioventricular connection is a rare congenital cardiac anomaly with many possible associated intracardiac and vascular pathologies such as hypoplastic ventricles, anomalies of the atrioventricular valves and malposition of the great arteries. The hallmark of the anomaly is non-parallel opening axes of AV valves. Features of this pathology maybe subtle but can be identified on CMR if the images are reviewed with a certain degree of suspicion. CMR is also a very good modality to investigate possible associated pathologies.
References:
1. Yoo SJ, Seo JW, Lim TH, Park IS, Hong CY, Song MG, Kim SH, Choe KO, Cho BK, Lee HJ. Hearts with twisted atrioventricular connections: findings at MR imaging. Radiology, 1993 Jul;188(1):109-13
2. Fyler DC. Trends. In Nada’s Pediatric Cardiology, FylerDC (ed). Hanley & Belfus: Philadelphia, PA, 1992; 273–280
3. Anderson RH, Baker EJ, Penny D, Redington AN, Rigby ML, Wernovsky G (2010) Paediatric Cardiology. Churchill Livingstone, Elsevier, Philadelphia.
COTW handling editor: Sylvia Chen
Have your say: What do you think? Latest posts on this topic from the forum

