



Case from: Joseph Daoko1, M.D, F.A.C.C., Jon Krathen2, D.O.
Institute: Memorial Hospital, (1) Department of Cardiology and (2) Internal Medicine Departments, York, Pennsylvania, USA
Clinical history: A 53 year-old man with no significant past medical history presented to our hospital reporting severe substernal chest pressure with associated diaphoresis that woke him up from sleep at 3:30 a.m
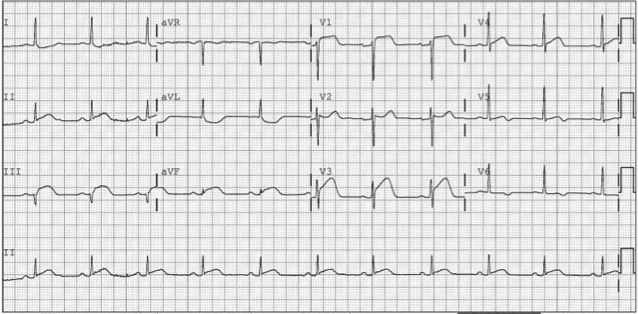
Figure 1
A standard 12-lead electrocardiogram (Figure 1) showed marked ST-segment elevation in leads V1, V2, and V3 and in the inferior leads II, III, and aVF, with ST depression in leads I, aVL, with T wave inversion in V5 and V6. The electrocardiogram findings suggested acute myocardial infarction of the inferior and septal walls.
The emergency department felt the patient had a STEMI, and urgent catheterization was indicated. The patient was given Aspirin as well as a Heparin bolus in the emergency room. He subsequently underwent an emergent cardiac catheterization.
Coronary angiography showed non-obstructive Coronary Artery Disease (CAD) of the mid right coronary artery and no clinically significant disease in the left coronary artery.
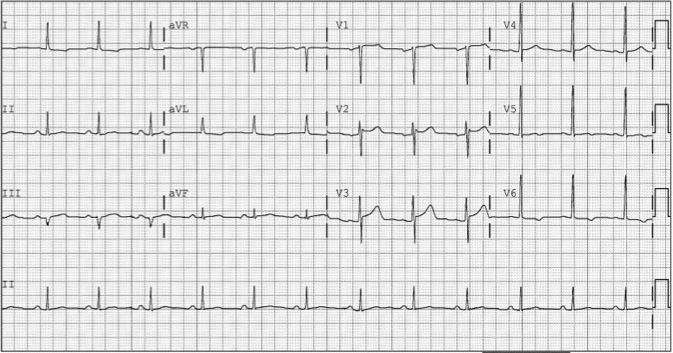
Figure 2
Cardiac markers were noted to be elevated (Tropnin-I 47.5 µg/L, CK 1456 mcg/L, CK-MB 172.21 ng/ml). The patient’s chest pain and EKG changes resolved (Figure 2).

Movie 4 & Movie 5
A 2-D echocardiography assessment reported normal LV function and wall motion. The right ventricle was not well visualized on the echocardiography (Movies 4 & 5).
CMR Findings:

Movie 6 & Movie 7
Cardiac gated steady-state free precession (SSFP) sequences showed severe hypo-kinesis of the inferior portion of the right ventricular free wall (Movies 6 & 7).
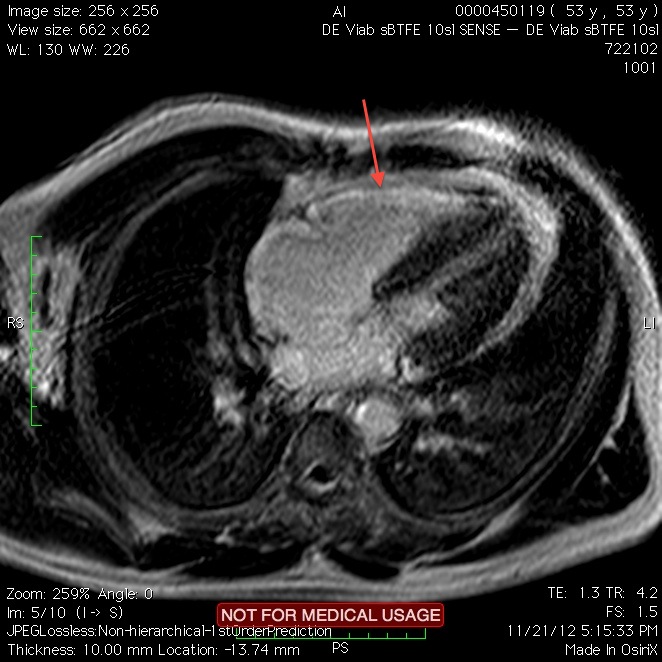
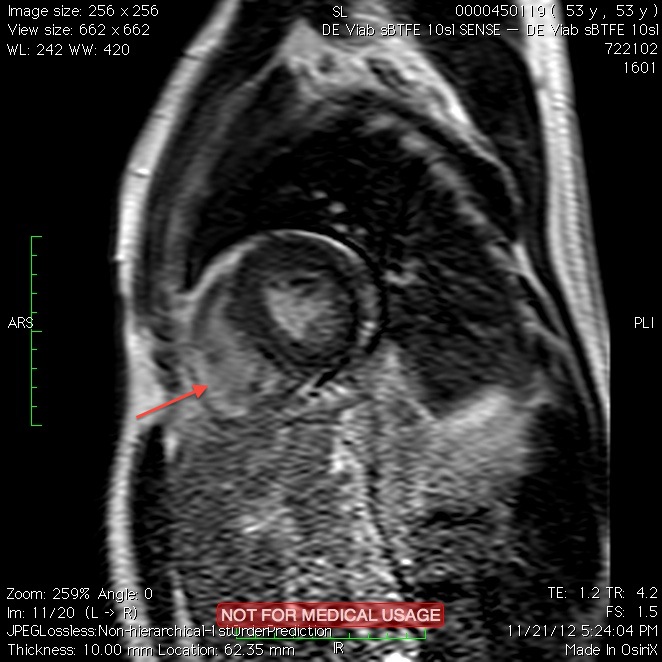
Figure 3 & Figure 4
Contrast-enhanced magnetic resonance imaging showed delayed hyperenhancement of the right ventricular (RV) free wall (arrows) without involvement of left ventricle (LV) (Figures 3 & 4).
The findings on the CMR were consistent with the presence of isolated right ventricular infarction that explained the EKG findings and the elevated cardiac markers.
Conclusion: The patient presented with symptoms and initial findings consistent with an inferior and septal transmural infarction. However, the coronary angiography did not show obstructive coronary artery disease. The patient likely had a spontaneous reperfusion. Cardiac MRI demonstrated an isolated right ventricular infarct, and it was crucial in establishing the diagnosis in this challenging case1.
Perspective: Isolated right ventricular myocardial infarction (RVMI) is rare, and accounts for only 3% of all infarctions. It is predominantly a complication of inferior myocardial infarction, or could be due to the occlusion of a nondominant right coronary artery (RCA) 2. The electrocardiographic changes may be misinterpreted as signs of infarction of the anterior wall because of the ST-segment elevation in leads V1-V2.
It has been reported as a complication of percutaneous coronary intervention involving the right coronary artery due to occlusion of the right ventricular branch3.
Our case, to the best of our knowledge, is the first reported case of isolated right ventricular myocardial infarction with ST elevation in the inferior and anterior leads without evidence of occlusive coronary artery disease on coronary angiography.
Of note, late gadolinium enhancement of the right ventricle can be very challenging, due in part to the relatively thinner myocardial wall of the right ventricle in comparison with the left ventricle. In this case, the short-axis late gadolinium enhancement image nicely demonstrates some right ventricular “nulling” as well as late gadolinium enhancement, and this imaging feature should be sought, in order to reduce over-calling of potential artifacts.
References:
1. Miszalski-Jamka T, Klimeczek P, Tomala M, et al. Extent of RV Dysfunction and Myocardial Infarction Assessed by CMR Are Independent Outcome Predictors Early After STEMI Treated With Primary Angioplasty. J Am Coll Cardiol Img. 2010;3(12):1237-1246
2. Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330:1211
3. Van der Bolt CL, Vermeersch PH, Plokker HW. Isolated acute occlusion of a large right ventricular branch of the right coronary artery following coronary balloon angioplasty. The only true ‘model’ to study ECG changes in acute, isolated right ventricular infarction. Eur Heart J 1996;17:247-50.
COTW handling editor: Monica Deac
Have your say: What do you think? Latest posts on this topic from the forum

