



Case from: Ashish Aneja MD1, Timothy Hoffman MD2, Sharon Roble MD1, Subha Raman MD MSEE1
Institute: 1. Ohio State University, Columbus, Ohio
2. Nationwide Children’s Hospital, Columbus, Ohio
Clinical history: A 19 year-old male presented for follow-up evaluation for cardiomyopathy following referral from a physician in West Virginia (Figure 1). Since his initial diagnosis of cardiomyopathy at the age of 2, he has remained asymptomatic from the cardiovascular standpoint. He denies any symptoms with ordinary exertion but had not undergone formal stress testing.
At age 2 years a murmur was detected and he underwent an echocardiography. Echocardiography at that time was notable for a left ventricular (LV) apical aneurysm and a mobile structure attached to the LV free wall. During systole, this protruded into the LV outflow tract and resulted in a dynamic gradient of 19-23mm Hg.
Following these abnormal findings he underwent a left and right cardiac catheterization. This invasive test demonstrated normal intra-cardiac pressures, normal coronary arteries and an absence of shunt physiology. The aorta, pulmonary arteries, and the right ventricle were also deemed normal by right ventriculography, pulmonary arteriography and an aortogram. The left ventriculogram was significantly abnormal with a cylindrical cavity, a dyskinetic apex and several band-like irregularities in the LV inflow.
Review of echocardiographic and cardiac catheterization data by several institutions yielded no diagnosis or specific management other than recommendation of antiplatelet therapy.
Family history consists of mitral valve prolapse in his mother. One of his two male siblings has been diagnosed with bicuspid aortic valve disease, and there was no history of sudden cardiac death or heart failure in first and second-degree relatives.
Cardiac magnetic resonance examination was requested to better define myocardial structure and cardiac function (Movie 1, Figure 2).
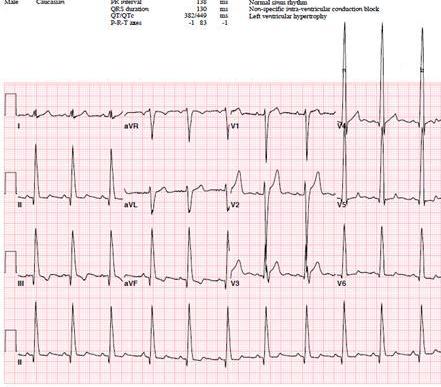
Figure 1: Resting 12 lead electrocardiogram
Movie 1a-d: Cardiac MRI cine images demontrating focal areas of hypertrophy consistent with sawtooth cardiomyopathy
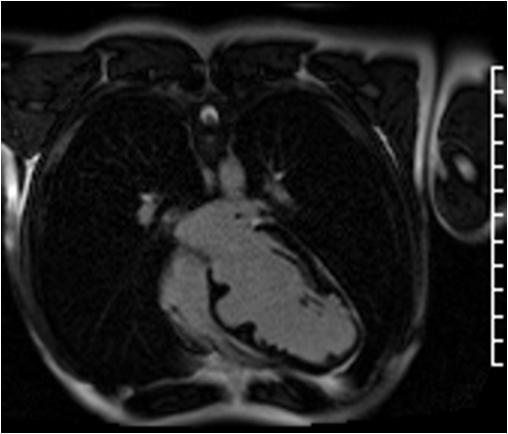
Figure 2: Myocardial delayed enhancement (PSIR) demonstrating the absence of prior infarct as a cause for myocardial thinning
Follow up: The patient continued to deny symptoms despite a follow up electrocardiogram and holter monitor which showed the presence of frequent ventricular ectopy, and non sustaind wide complex tachycardia which was felt to be ventricular tachycardia (Figure 3). He subsequently received a single chamber implantable cardiac defibrillator for primary prevention of sudden cardiac death.
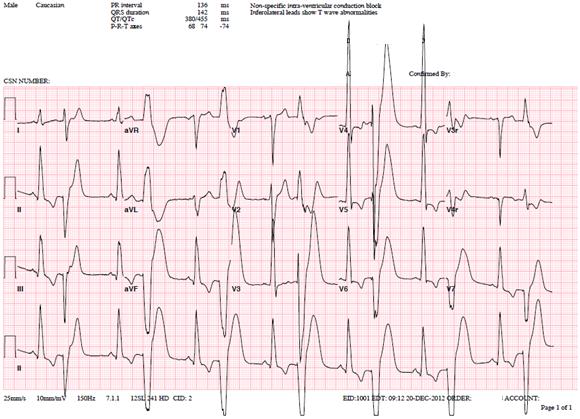
Figure 3: Follow up electrocardiogram demonstrating frequent ventricular ectopy
Conclusion: Sawtooth cardiomyopathy had been previously proposed as the diagnosis based on the patient’s prior invasive study. Disordered cardiac embryogenesis was also suspected. To date the patient has not received any therapies from his implantable cardiac defibrillator.
Perspective: While similar morphology has been previously described, underlying mechanisms of this unusual form of myocardial disease remains unknown.1 Further investigations that would be potentially informative, such as genetic testing and endomyocardial biopsy with precise characterization of ultrastructural abnormalities have not been pursued at this time.2
References:
1. Davlouros PA, Danias PG, Karatza AA, Kiaffas MG, Alexopoulos D. Saw-tooth Cardiomyopathy. J Cardiovasc Magn Reson 2009;11:54.
2. Harvey PA, Leinwand LA. The Cell Biology of Disease: Cellular Mechanisms of Cardiomyopathy. J Cell Biol. 2011 Aug 8;194(3):355-65.
COTW handling editor: Kevin Steel
Have your say: What do you think? Latest posts on this topic from the forum