



Case from: Heiko Kindler, Ricardo Wage, Gerard King, John Clarke.
Institute: Eagle Lodge Centre for Advanced Cardiovascular Imaging, Limerick and Dublin, Ireland
Clinical history: A 70-year male presented with gradual deterioration, breathlessness, and peripheral oedema as well as bilateral pleural effusions. He had previous CABGx4(LIMA LAD, VG to OM, Diagonal and RCA). ECG showed small QRS voltages, septal Q waves, poor R wave progression (Figure 1) Echocardiography suggested a speckled appearance of the myocardium and basal-mid inferior hypokinesis. CMR shows bilateral pleural effusions, LVH, widespread LV and RV enhancement in a subendocardial pattern and inferior/lateral microvascular obstruction (MVO). A CT coronary angiogram confirmed PDA graft insertion stenosis.
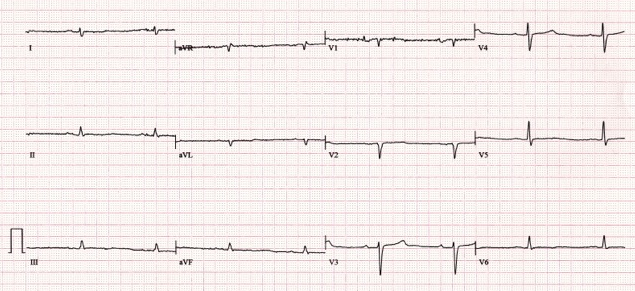
Figure 1
CMR Findings: SSFP Cine images show a dilated LV with severe impairment (LVEF 36%) global hypertrophy (maximum LV wall thickness 16mm), bi-atrial dilatation and bilateral pleural effusions. (Movie 1 and 2)
Early gadolinium phase: Micro-Vascular Obstruction, MVO In the early phase after gadolinium injection the perfused myocardium and left ventricular cavity appears relatively high in signal. A large dark area (low signal intensity on T1 weighted imaging) perfusion defect appears at the infero-septal, inferior and infero-lateral segments which is characteristic of MVO. (Figure 2)
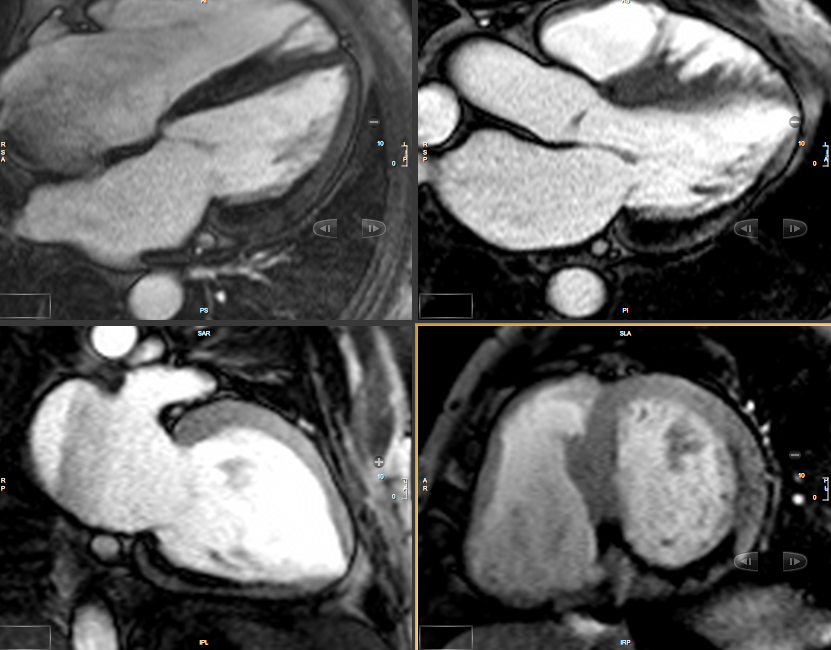
Figure 2
Late phase after Gadolinium injection: Global LV and RV enhancement in a subendocardial distribution pattern. In cardiac amyloidosis, CMR imaging demonstrates a characteristic pattern of global subendocardial late enhancement combined with abnormal myocardial and blood-pool kinetics. (figure 3 and 4)
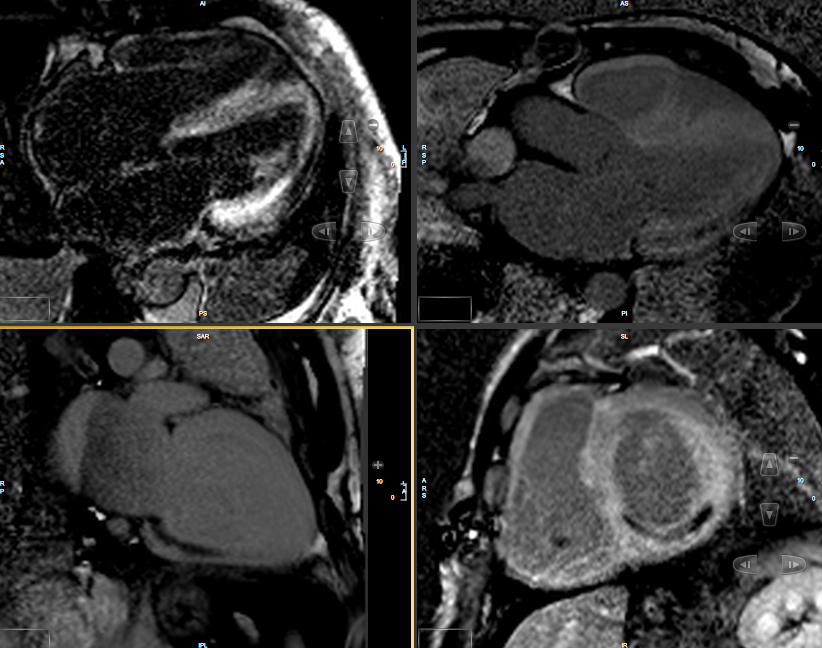
Figure 3
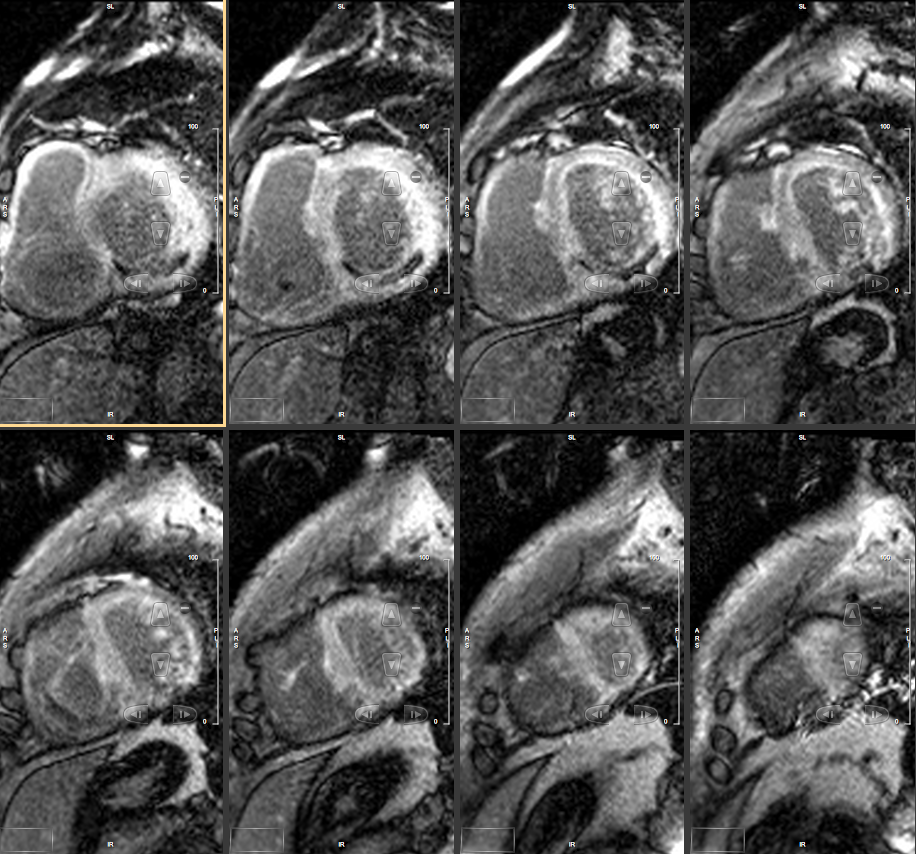
Figure 4
CT Coronary Angiography: The LIMA – LAD and both vein grafts to Circumflex and Diagonal arteries are patent. There is abrupt discontinuation of contrast opacification at the point of vein graft insertion to the distal RCA/PDA (arrows on figure 5-7 and 3D movie)

Figure 5
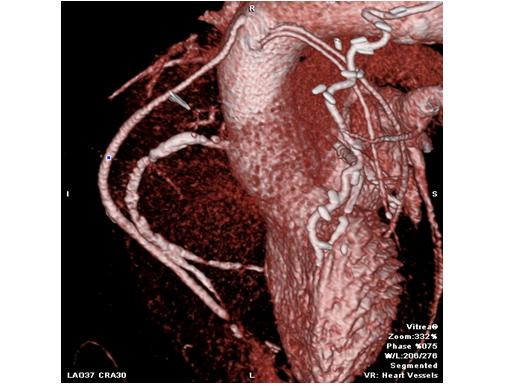
Figure 6

Figure 7
Movie 3D
Perspective:
This case illustrates the additional value of a CMR/CTA multimodality imaging ‘one stop shop’. The time taken for acquisition of both scans was less than 60 minutes in a patient who was betablocked and in sinus rhythm.
The early phase of gadolinium enhancement can reveal avascular structures such as thrombus of the left ventricle, left atrium and the left trial appendage. In this particular case we demonstrate a marked resting perfusion defect caused by recent graft occlusion. The discovery of specific patternsof late enhancement in Cardiac Amyloidosis has lead to the recognition of CMR as the test of choice in myocardial involvement of many conditions. The characteristic pattern of enhancement is considered to be highly characteristic of amyloidosis (1)may be seen in the familial form of Cardiac Amyloid (Transthyretin, TTR mutation). The second characteristic feature in the late phase of gadolinium enhancement is a dark blood pool, a phenomenon related to abnormal gadolinium kinetics (figures 2 and 3).Thelate enhancement pattern in Amyloidosis has been shown to correlate well with tissue samples on biopsy and post mortem examinations (4). In one study it was found to be superior to other “conventional predictors of mortality”(5)
CMR delivers highly specific, high resolution imaging of perfusion defects. It provides detailed differential diagnostic information, as in this case of a new diagnosis of heart failure due to Cardiac Amyloidosis with acute deterioration resulting from bypass graft occlusion and microvascular obstruction.
The advantage of having a Multi-slice detector Coronary CTAngiography in close proximity facilitates the non-invasive assessment of complex coronary anatomy in patients with bypass grafts.
Scanners used: CMR Siemens MAGNETOM® Espree1.5T, 70cm bore, 125cm Z axis length, Contrast: Gadovist (1.0 mmol/mL solution of 10-(2,3-Dihydroxy-1 hydroxymethylpropyl)-1,4,7,10-tetraazacyclododecane-1,4,7-triaceticacid)CTAToshiba Aquilion One 320 slice MDCT; Contrast 50-60ml Niopam 370, prospective gating.
Image Analysis Post processing CMR:For quantitative measures of left and right ventricular function, stroke volume and ejection fraction and mass index SSFP images were analyzed using dedicated cardiac software (CMR 42, Circle Cardiovascular Imaging Inc). CTA:Vitrea Workstation, Toshiba Medical Systems.
References:
- Maceira AM, Joshi J, Prasad, SK. Cardiovascular Magnetic Resonance in Cardiac Amyloidosis. Circulation. 2005; 111: 186-193
- VandenDriesen RI, Slaughter, RE, Strugnell, WE. MR Findings in Cardiac Amyloidosis. American Journal of Roentgenology. 2006;186:1682-168
- Kyle RA, Greipp PR, O’Fallon WM. Primary systemic amyloidosis: multivariate analysis for prognostic factors in 168 cases. Blood. 1986; 68: 220–224.
- Vogelsberg H, Mahrholdt H, Deluigi CC, Yilmaz A, Kispert EM, Greulich S, Klingel K, Kandolf R, Sechtem U. Cardiovascular magnetic resonance in clinically suspected cardiac amyloidosis: noninvasive imaging compared to endomyocardial biopsy. J Am CollCardiol. 2008; 51: 1022–1030
COTW handling editor: Dr Giovanni Quarta

