



Case from: Johanne Neill1 , Lou Hofmeyr1, Wendy Strugnell1, Allan Wesley1, Christian Hamilton-Craig1,2
Institute: 1. The Richard Slaughter Centre of Excellence in Cardiovascular MRI, Prince Charles Hospital, Brisbane, QLD, Australia. 2. University of Queensland, Brisbane, Australia.
Clinical history:
A 44 year old male status-post repair of dextro-transposition of the great arteries presented with atypical chest pain in the context of hypertension and hypercholesterolaemia. His d-transposition had been surgically treated with a Senning atrial switch repair. With the exception of occasional paroxysms of atrial fibrillation he had been stable for many years. There were no significant findings on clinical examination. The clinical team wished to evaluate the cardiac anatomy, the baffle connections and also assess stress myocardial perfusion for possible coronary artery disease. A comprehensive CMR protocol was performed including bSSFP imaging, phase contrast flow quantitation, free-breathing motion corrected adenosine stress first pass perfusion imaging and late gadolinium enhancement.
CMR Findings: The study was performed on a Siemens Aera 1.5 Tesla magnet, demonstrating patent atrial baffles, and a severely hypertrophied and dysfunctional systemic right ventricle with normal subpulmonic ventricular function.

Movie 1 – Steady state free precession TruFISP axial stack (1.27ms TE/ 42.42 ms TR/ 8mm thickness) demonstrating the cardiac anatomy of repaired d-transposition with Senning baffles. The morphological left subpulmonic ventricle is normal in size and function. The pulmonary venous connections to the right atrium are widely patent. The morphological right systemic ventricle is significantly hypertrophied with an ejection fraction of 27%.

Movie 2 – Balanced steady state free precession series demonstrating that the superior and inferior vena caval baffles to the left atrium are widely patent.

Movie 3 and 4 – A free breathing, motion corrected TurboFLASH adenosine stress first pass perfusion series (1.17ms TE/167.6ms TR/100msTI/8mm thickness) in the ventricular short axis and a single long-axis view demonstrate homogeneous perfusion throughout the right and left ventricular myocardium.
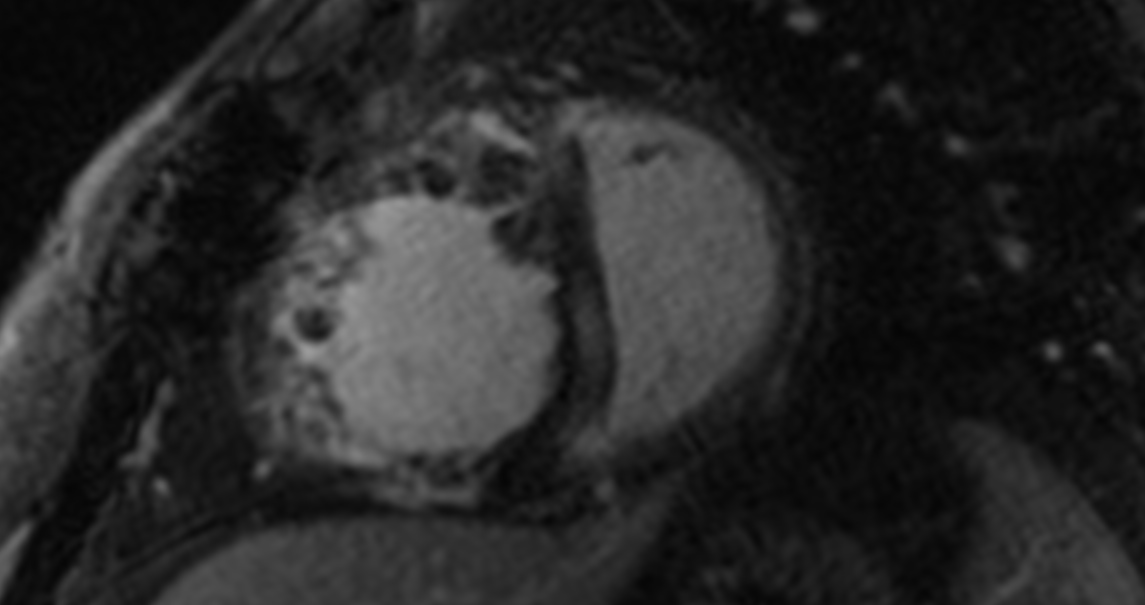
Figure 1 – The late gadolinium enhancement images demonstrate mid wall enhancement in the septum and the adjacent right ventricular myocardium secondary to chronic pressure load on the morphological right ventricle.
Conclusion: Cardiac MRI with first pass perfusion was able to address a number of clinical questions in this man with complex anatomy. The use of gadolinium first pass during adenosine stress MRI to assess a systemic right ventricle has not been described. Free-breathing motion-corrected perfusion imaging has significant advantages for ease of acquisition, high image quality, no Gibbs’ ring artifact, and high temporal and spatial resolution.
Perspective: Systemic right ventricles are at high risk of contractile dysfunction, the cause of which is still unclear. The chronic exposure of the morphological right ventricle to systemic pressure leads to significant hypertrophy. Ischaemia has been postulated to contribute to the right ventricular systolic dysfunction by a number of mechanisms. Supply demand mismatch from an inadequate coronary circulation to support the hypertrophied right ventricle may contribute. In addition, systemic arterial hypoxaemia in the preoperative period and the cardiopulmonary bypass for correction may damage the RV myocardium1, 2, 3.
Small numbers of paediatric and adult patients with systemic right ventricles have been studied using myocardial perfusion single photon emission tomography (SPECT) with Sestamibi. A variety of fixed and inducible perfusion defects have been described and believed to be associated with the degree of right ventricular dysfunction and the delay to corrective surgery 2, 3. Myocardial perfusion scintigraphy is not ideally suited for this purpose. Only by virtue of hypertrophy can the right ventricle be visualised at all; the patterns and effect of attenuation on right ventricular assessment are therefore not well known.
Evaluation of these patients by adenosine stress first pass perfusion cardiac MRI has several advantages over SPECT. Cardiac MRI is the gold standard imaging method for assessment of right ventricular anatomy and function. The improved spatial resolution of cardiac MRI over SPECT allows better identification of subendocardial perfusion abnormalities4. The additional anatomical and functional information available from a cardiac MRI is clinically useful in these complex patients. Clearly no radiation is used in cardiac MRI compared with typical doses of approximately 10mSv in Sestamibi SPECT.
This comprehensive MRI protocol was able to demonstrate an unobstructed Senning repair and an impaired, hypertrophied systemic right ventricle with no suggestion of epicardial coronary flow limitation or global subendocardial ischaemia or infarction. The cause of the right ventricular dysfunction in this case is non-ischaemic ventricular dysfunction, likely from chronic pressure overload of the systemic right ventricle which is supported by the pattern of late gadolinium enhancement. Cardiovascular MRI was able to fully assess this complex patient in a single examination without ionizing radiation.
References:
- Sunduram PS, Padma S. Role of myocardial perfusion single photon emission computed tomography in pediatric cardiology practice. Annals of Pediatric Cardiology 2009; 2(2):127-139.
- Lubiszewska B, Gosiewska E, Hoffman P, Teresinska A, Rozianski J, Piotrowski W, Rydlewska-Sadowska W, Kubicka K, Ruzytto W. Myocardial perfusion and function of the systemic right ventricle in patients after atrial switch procedure for complete transposition: long term follow-up. Journal of the American College of Cardiology 2000; 36:1365-1370.
- Hornung TS, Bernard EJ, Jaeggi ET, Howman-Giles RB, Celermajer DS, Hawker RE. Myocardial perfusion defects and associated systemic ventricular dysfunction in congenitally corrected transposition of the great arteries. Heart 1998; 80:322-326.
- Prakash A, Powell AJ, Krishnamurthy R, Geva T. Magnetic resonance imaging evaluation of myocardial perfusion and viability in congenital and acquired pediatric heart disease. The American Journal of Cardiology 2004; 93:657-661.
Disclosures: Dr Hamilton-Craig is supported by the Smart Futures Fellowship, Queensland Government. No conflicts of interest.
COTW handling editor: M. Jay Campbell, MD