



Case from: David Parra, Jon Soslow, Vernat Exil, Neeru Kaushik
Institute: Vanderbilt University Medical Center, Department of Pediatrics, Division of Pediatric Cardiology, Nashville, TN.
Clinical history:
A 3 year old girl was evaluated in clinic with a history of a previously diagnosed right aortic arch and a patent ductus arteriosus. Her chief complaint was occasional emesis with feeds, but with adequate weight gain. She had no respiratory symptoms such as stridor or wheezing, and there were no signs or symptoms of congestive heart failure. Her echocardiogram confirmed the diagnosis of a right aortic arch and a patent ductus arteriousus, however the branching of the arch was not determined and an aberrant left subclavian artery was suspected.
CMR Findings:
CMR was performed on a 1.5T Philips Intera MRI scanner to delineate the anatomy with suspicion of a vascular ring.
Movie 1: ECG gated SSFP images in axial plane through the thorax demonstrate isolation of the left subclavian artery off the main pulmonary artery and a right aortic arch (movie 1).

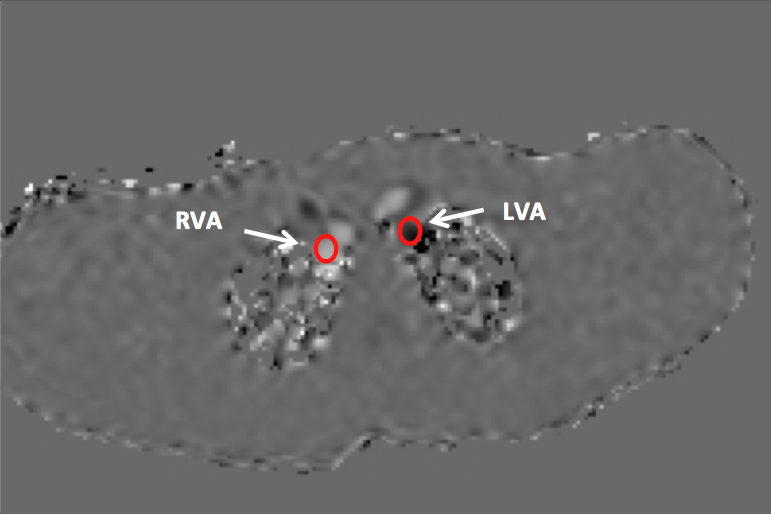
Movies 2 and 3; Figure 1: ECG gated SSFP axial images (movie 2) and corresponding velocity encoded imaging through plane at the level of the right and left vertebral arteries simultaneously depicting flow in the cranial direction in the right carotid and vertebral artery and flow in the caudal direction (retrograde)in the left vertebral indicating steal phenomenon (movie 3). Figure 1 is a still frame velocity encoded imaging through plane image labeling the vessels of interest. RVA=right vertebral artery. LVA=left vertebral artery.
Movie 4: 3D volume rendered reconstruction of an ECG gated contrast enhanced angiogram demonstrates the origin of the isolated left subclavian artery and the presence of a larger caliber right vertebral artery and prominent collaterals at the level of circle of Willis (movie 4).
Conclusion:
CMR reveals not only the anatomic diagnosis of isolated left subclavian artery from the main pulmonary artery, but also highlights the physiologic component of suclavian steal phenomenon in this case.
Perspective:
Isolation of the left subclavian artery from the main pulmonary artery is an uncommon arch anomaly (1). It can be embryologically explained using Edwards hypothetical double aortic arch model where the left aortic arch is interrupted proximal to the left common carotid artery by involution of the left fourth arch with a second interruption distal to the left sixth arch by involution of the distal left dorsal aorta. This leaves the left subclavian artery connected to the pulmonary artery through the ductus arteriosus(2). Subclavian steal may occur, as in this case, by flow down the vertebral artery through the ductus into the low resistance pulmonary artery (3,4)
The diagnosis of subclavian steal by a combination of angiography, phase contrast MRI and Doppler ultrasonography in adults has been reported in the literature (5). This case identifies the utility of CMRI in the diagnosis of subclavian steal in this unusual aortic arch anomaly.
References:
1. Leutmer PH, Miller GM. Right aortic arch with isolation of the left subclavian artery: case report and review of the literature. Mayo Clin Proc 1990; 65:407-413.
2. Weinberg P. Aortic arch anomalies: In: Allen H, Gutgesell H, Clark E, Driscoll D, editors. Moss and Adams’ Heart Disease in Infants, Children, and Adolescents. Philadelphia: Lipincott Williams&Wilkins; 2001. p. 707-735.
3. Reeves BM, Colen TM, Sheridan BJ, Ward C. Isolated innominate artery as a cause of subclavian steal and cerebral hemisphere atrophy. Pediatr Cardiol 2010; 31:1083-1085.
4. Fulwani MC, Vajifdar B, Kukarni SM, Dalvi BV. Isolated innominate artery in association with patent ductus arteriosus and left pulmonary arterial ostial stenosis. Indian Heart J 1998. 50: 206-208.
5. Akin K, Kosehan D, Kirbas I, Yildirim M, Koktener A. Diagnosis and percutaneous treatment of partial subclavian steal: Doppler ultrasonography and phase contrast magnetic resonance angiography findings and a brief review of the literature. Jpn J Radiol 2011; 29:207-211.
COTW handling editor: M. Jay Campbell, MD
Have your say: What do you think? Latest posts on this topic from the forum