



Case from: Sarai Roche MD1, Victor Pineda MD1, Hug Cuellar MD1, Jose Rodriguez-Palomares MD2
Institute: Hospital Universitari Vall d’Hebrón, Barcelona, Spain – 1 Radiology Department; 2 Cardiology Department.
Clinical history: A 77-year-old immuno-competent man was referred to our emergency room for onset of dyspnea, orthopnea and paroxysmal nocturnal dyspnea. His medical history included adenocarcinoma of the sigmoid colon 7 years earlier, treated with tumor resection and adjuvant chemotherapy, and undifferentiated gastric adenocarcinoma 3 years previously that had been treated with total gastrectomy and showed no evidence of disease on follow-up. The patient denied use of alcohol, drugs or medication except pharmacological treatment for dyslipidemia and hypertension.
A physical examination revealed jugular vein engorgement and bilateral lower extremity edema. Laboratory tests revealed normocytic anemia, hypocalcemia, hypoproteinemia and elevated levels of fibrinogen and LDH (630 U/L ; normal levels 216-360 U7L). CA 125 was also elevated (53 U/ml ; normal levels <35 U/ml), the remaining tumor marker levels including CEA, CA19.9 and CA72.4 were normal.
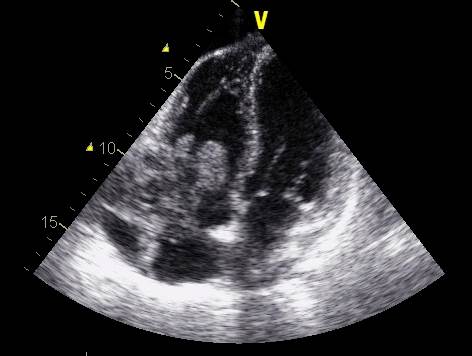
Figure 1
A transthoracic echocardiography demonstrated a large heterogeneous mass in the right-sided cardiac chambers, near the tricuspid annulus, causing functional valvular stenosis. (Fig 1).
CMR Findings:
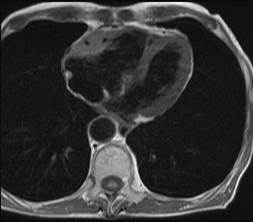
Figure 2
Cardiac magnetic resonance (CMR) imaging showed a solid tumor in the right atrioventricular groove that was iso-intense with respect to myocardium on TSE T1-weighted images (Fig 2).
Figure 3 – Movie 1
The mass surrounded the right coronary artery without causing occlusion and invaded the right atrial wall. The lesion was also iso-intense/slightly hyper-intense in comparison to myocardium on cine-MR sequences. In addition, an extensive mobile mass – possibly corresponding to a thrombus – was detected in the right atrium on these sequences (Fig 3, movie 1).
Figure 4 – Movie 2
Following contrast administration, the lesion showed mild homogeneous enhancement during the perfusion sequence (Fig 4, movie 2). Of note, the thrombus lacked any enhancement.
Conclusion: In light of these imaging findings, a differential diagnosis of metastasis, lymphoma, and primary sarcoma was established, with cardiac lymphoma being considered the first option.
The key imaging findings that suggested lymphoma as the first diagnostic option were the location of the lesion in the right atrioventricular groove, the absense of tumor necrosis, the presence of an intra-atrial thrombus, and particularly, the relationship of the mass with the right coronary artery which was enveloped by the mass, but showed no occlusion or stenosis (typical of lymphoma in other locations). Metastases to the heart and pericardium are much more common than primary cardiac tumors but tend to occur late in the course of a malignant disease when the patient typically has metastatic disease at other sites. In general, cardiac sarcomas are known to have more necrosis or hemorrhage than lymphomas so the signal intensity of sarcomas is more heterogeneous.
The patient underwent US-guided cardiac biopsy, but the material obtained was not sufficent to establish the diagnosis. Ultimately, tumor biopsy via median sternotomy confirmed the diagnosis of primary cardiac lymphoma (large B-cell lymphoma). Bone marrow biopsy and thoraco-abdominal CT showed no extracardiac involvement and particularly, there were no signs of nodal or extranodal involvement. Following chemotherapy treatment, a repeat CMR two months later showed a significant reduction in tumor size.
Perspective: Primary tumors of the heart are uncommon, and up to 75% are benign. Malignant primary tumors of the heart are predominantly of sarcomatous lineage of which primary cardiac lymphomas are extremely rare [1], accounting for only 1.3% of primary cardiac tumors [2]. By definition, primary cardiac lymphoma exclusively affects the heart and pericardium, with no evidence of extracardiac disease [3]. It is usually an aggressive B-cell lymphoma occurring in an immune-depressed patient. Symptoms may vary according to the side of the heart that is involved; the most frequent ones are unresponsive right heart failure, arrhythmia, chest pain and pericardial effusion [4].
However the clinical-analytic presentation is non-specific; hence imaging techniques are needed to reach a diagnosis. Cardiac magnetic resonance is the reference technique for evaluating cardiac tumors, with the ability to determine their location, characterization, and impact on heart function [1]. They commonly present as multiple nodular masses infiltrating the myocardium and showing heterogeneous contrast uptake, or as a diffuse pericardial infiltration with associated pericardial effusion [2]. The involvement of the right atrium, absence of tumor necrosis, presence of pericardial effusion, and valve preservation have been described as signs suggestive of cardiac lymphoma rather than other primary cardiac tumors [3].
With this case we would like to emphasize that in addition to the findings classically described suggesting cardiac lymphoma, an important radiologic feature was the predilection for the atrioventricular groove, and particularly, the relationship of the mass with the right coronary artery which was enveloped by the mass, but showed no occlusion or stenosis (typical of lymphoma in other locations). We encountered this finding in another case of cardiac lymphoma in our center as well as in cases described in the literature, and we consider this a useful radiologic sign for the differential diagnosis of cardiac masses suggesting primary cardiac lymphoma.
References:
1. Randhawa K, Ganeshan A, Hoey ET. Magnetic resonance imaging of cardiac tumors: part 1, sequences, protocols, and benign tumors. Curr Probl Diagn Radiol. 2011; 40:158-68.
2. Randhawa K, Ganeshan A, Hoey ET. Magnetic resonance imaging of cardiac tumors: part 2, malignant tumors and tumor-like conditions. Curr Probl Diagn Radiol. 2011; 40:169-79.
3. Araoz PA, Eklund HE, Welch TJ. Breen JF. CT and MR imaging of primary cardiac malignancies. Radiographics 1999; 19:1421-34.
4. Miguel CE, Bestetti RB. Primary cardiac lymphoma. Int J Cardiol 2011; 149(3):358-63.
COTW handling editor: Monica Deac, MD
Have your say: What do you think? Latest posts on this topic from the forum

