



M. Jay Campbell, M.D.1,2; Stephen Darty2; Michael Carboni, M.D.1; Louis Dibernardo, M.D.3; Piers C.A. Barker, M.D.1,2
Duke University Department of Pediatrics1, Duke Cardiovascular Magnetic Resonance Center2, Duke University Department of Pathology3
Clinical Presentation:
The patient’s mother presented at 33 weeks gestation for a fetal echocardiogram secondary to a suspected cardiac abnormality on obstetrical ultrasound. The fetal echocardiogram revealed a large cardiac mass in the interventricular septum (Movie 1 and Image 1), premature ventricular contractions, and a small pericardial effusion. The patient’s mother developed pre-eclampsia at 34 weeks and underwent an emergent Caesarean section.
Movie 1: Fetal echocardiogram, four chamber axial cine revealing a large cardiac mass in the interventricular septum.
Image 1: Fetal echocardiogram, four chamber axial image revealing a large cardiac mass which
measured 2.8 x 1.5 cm.
The 2110 gram female patient was admitted to the neonatal intensive care unit. She was hemodynamically stable. A transthoracic echocardiogram was performed and revealed a large, well circumscribed cardiac mass involving the left ventricular inferior, septal and lateral walls. (Movies 2 and 3) There was no obstruction to ventricular inflow or outflow tracts.
Movie 2: Transthoracic echocardiogram subcostal sagittal image revealing a large cardiac mass involving the inferior, septal and lateral walls of the left ventricle.
Movie 3: Transthoracic 3D full volume cine of the left ventricle illustrating a large left ventricular mass.
A cardiac MRI was performed under general anesthesia to evaluate the extent of the mass and its tissue characteristics. The cardiac MRI confirmed the presence of a large well circumscribed intra-myocardial mass originating from the inferior wall and extending into the septal and lateral walls. The mass extended from just below the annulus of the mitral valve to the apex. (Movies 4-6) There was no obstruction to ventricular inflow or outflow tracts. The mass was hypointense on cine imaging (Movies 4-6). Perfusion imaging revealed that the mass was not highly vascular (Movie 7). Late gadolinium delayed enhancement imaging was performed and revealed hyperenhancement of the border with a dark core (Image 2). T1 weighted fat saturation images were performed and did not indicate a lipoma. These CMR characteristics were consistent with a diagnosis of fibroma [1, 2].
Movies 4-5: Cine CMR images in the four chamber or axial view and the short axis view illustrating a large cardiac mass.
Movie 6: Cine CMR image of the left ventricle in a long axis view illustrating a large cardiac mass.
Movie 7: Perfusion CMR image of the left ventricle in a long axis view illustrating diminished perfusion of the cardiac mass.

Image 2: Late gadolinium delayed enhancement long axis image of the cardiac mass indicating a hyperintense border and a dark core
The patient initially did well but eventually began to develop symptoms of heart failure. Surgical resection was not felt to be a viable option given the large size of the mass. The patient underwent cardiac transplantation at 6 months of age. Gross and histological evaluation of the cardiac mass confirmed a diagnosis of a single large cardiac fibroma.
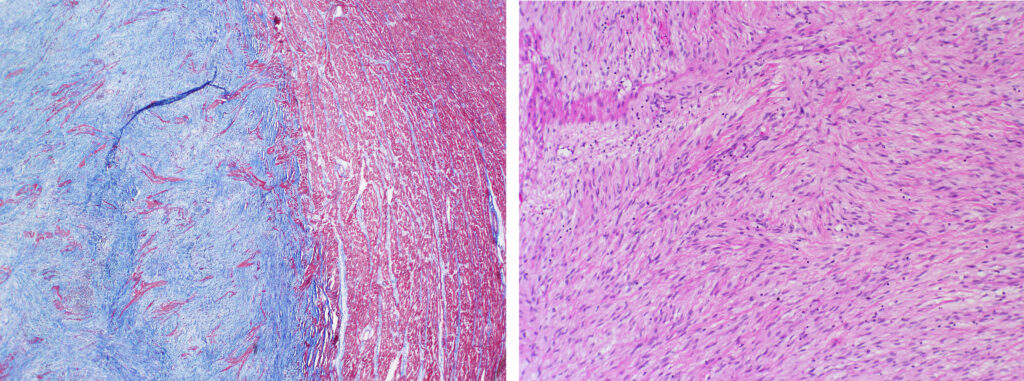
Images 3-4: Illustrate the characteristic histological appearance of a fibroma in this patient.
Cardiac masses in children are rare and most are benign [3]. The most common type is rhabdomyoma which is commonly associated with tuberous sclerosis [4]. The second most common is fibroma [5]. Fibromas are large, intramyocardial and usually occur in the ventricular septum and lateral wall [6]. Histologically, they consist of fibroblasts, collagen fibers, minimal elastic tissue and occasionally calcium deposits [6]. The clinical presentation is dependent on the mass’ effect on cardiac output and arrhythmia. Treatment can include observation, anti-arrhythmic medications, surgical resection and cardiac transplantation.
Cardiac MRI can be used to define the tissue characteristics of pediatric cardiac masses [1, 2]. Beroukhim et al. evaluated the tissue characteristics of pediatric cardiac masses and proposed a diagnostic prediction model [1]. Beroukhim’s model was applied to the MRI images in this case to make the correct diagnosis.
Click here to view all CMR images for the case on CloudCMR.
References:
1. Beroukhim RS, Prakash A, Buechel ER, Cava JR, Dorfman AL, Festa P, Hlavacek AM, Johnson TR, Keller MS, Krishnamurthy R, Misra N, Moniotte S, Parks WJ, Powell AJ, Soriano BD, Srichai MB, Yoo SJ, Zhou J and Geva T. Characterization of cardiac tumors in children by cardiovascular magnetic resonance imaging: a multicenter experience. Journal of the American College of Cardiology. 2011;58:1044-54.
2. Grizzard JD and Ang GB. Magnetic resonance imaging of pericardial disease and cardiac masses. Magnetic resonance imaging clinics of North America. 2007;15:579-607, vi.
3. Nadas AS and Ellison RC. Cardiac tumors in infancy. The American journal of cardiology. 1968;21:363-6.
4. Tworetzky W, McElhinney DB, Margossian R, Moon-Grady AJ, Sallee D, Goldmuntz E, van der Velde ME, Silverman NH and Allan LD. Association between cardiac tumors and tuberous sclerosis in the fetus and neonate. The American journal of cardiology. 2003;92:487-9.
5. Freedom RM, Lee KJ, MacDonald C and Taylor G. Selected aspects of cardiac tumors in infancy and childhood. Pediatric cardiology. 2000;21:299-316.
6. Fernando SS. Cardiac fibroma (fibrous hamartoma) of infancy. Two case reports. Pathology. 1979;11:111-7.

