



Dominique de Waard BSc, David Horne MD, Santokh Dhillon MD
Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia
Isaac Walton Killam Children’s Hospital, Halifax, Nova Scotia
Case Published in the Journal of Cardiovascular Magnetic Resonance: Click here for the link
Click here for PubMed Reference to Cite this Case
Clinical History:
An asymptomatic 10-year-old male visited his pediatrician for his regular attention deficit and hyperactivity disorder (ADHD) follow-up. A new systolic ejection murmur was heard. Chest x-ray showed an abnormal aortopulmonary window with enlargement of the left atrial shadow. ECG showed P-mitrale (M-shaped P-waves) in lead II and biphasic P-waves in lead V1, suggesting left atrial enlargement (Figure 1). These results prompted a referral to pediatric cardiology. Physical examination revealed a dynamic precordium, a loud first heart sound, a II/VI systolic ejection murmur variable in intensity with inspiration, and an early, high pitched diastolic plop sound at the apex after the second heart sound. Echocardiogram (Movie 1 and 2) revealed a large, mobile, homogeneous mass in the dilated left atrium. The mass appeared to be pedunculated, but CMR was sought for further investigation.
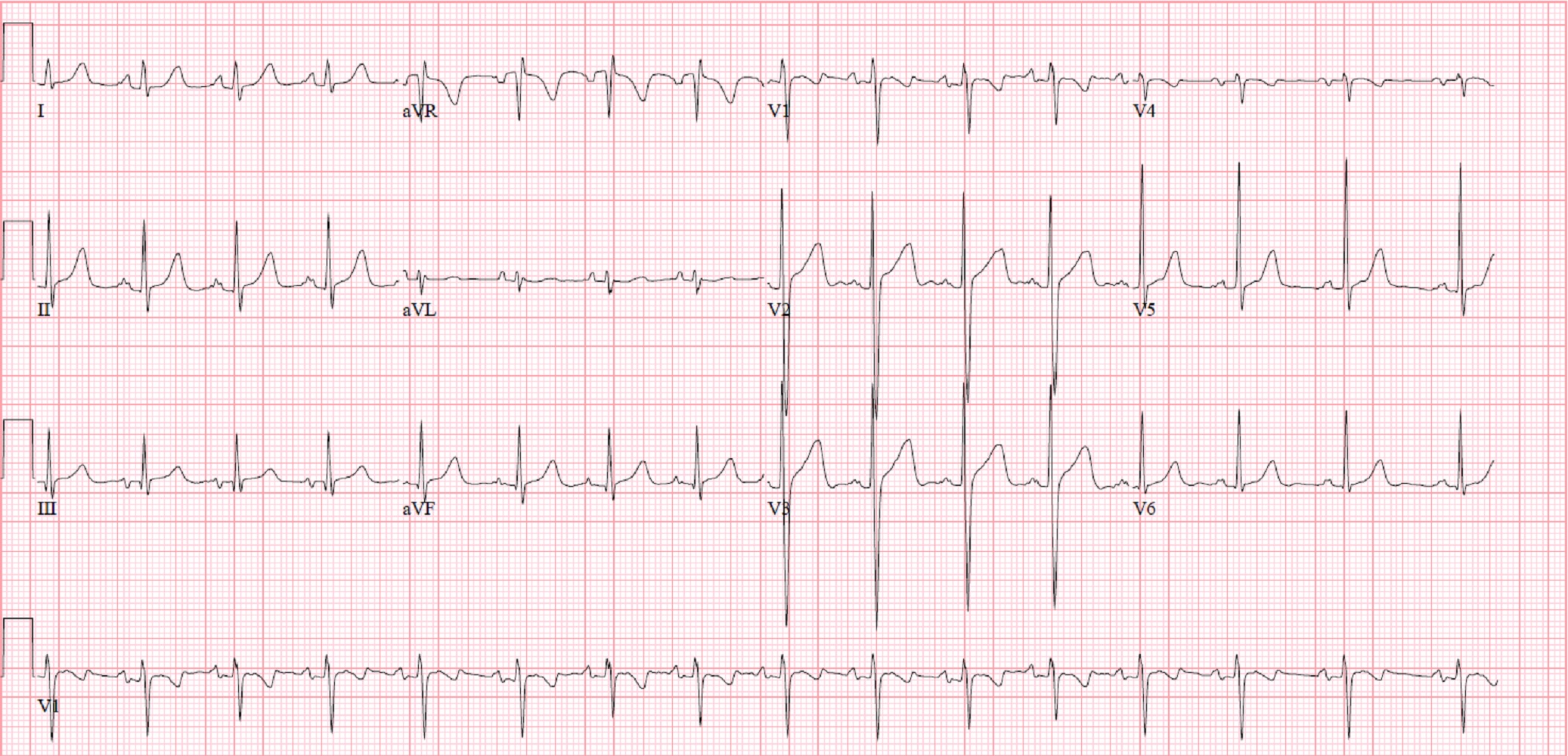
Figure 1. ECG showing signs of left atrial enlargement
Movie 1. Transthoracic echocardiogram parasternal long axis with color Doppler showing obstruction of mitral valve inflow from the mass and mitral valve insufficiency.
Movie 2. Transthoracic echocardiogram four chamber showing the left atrial mass extending past the mitral valve annulus during diastole.
CMR Findings
The cine SSFP short axis view clearly demonstrates a large, smooth, pedunculated and mobile mass (Movie 3). T1 with fat saturation and T2 imaging both showed hyperintensity (Figure 2 & 3, respectively). There was also hypointensity on first pass myocardial perfusion (Figure 4). All of these findings were in keeping with a probable diagnosis of a benign myxoma on CMR (1). On myocardial delayed enhancement (Figure 5) there was variable intensity, which could be an India ink artifact. With a higher inversion time, a myxoma would appear homogenous.
Determining the diagnosis of a left atrial myxoma, exact location of the stalk, proximity of the myxoma to the pulmonary veins (Movie 4), and the effects of the tumor on the mitral valve (Movie 5) were integral in preparation for surgery.
Movie 3. Short axis cine SSFP showing a large, relatively smooth, pedunculated mass attached to the interatrial septum.
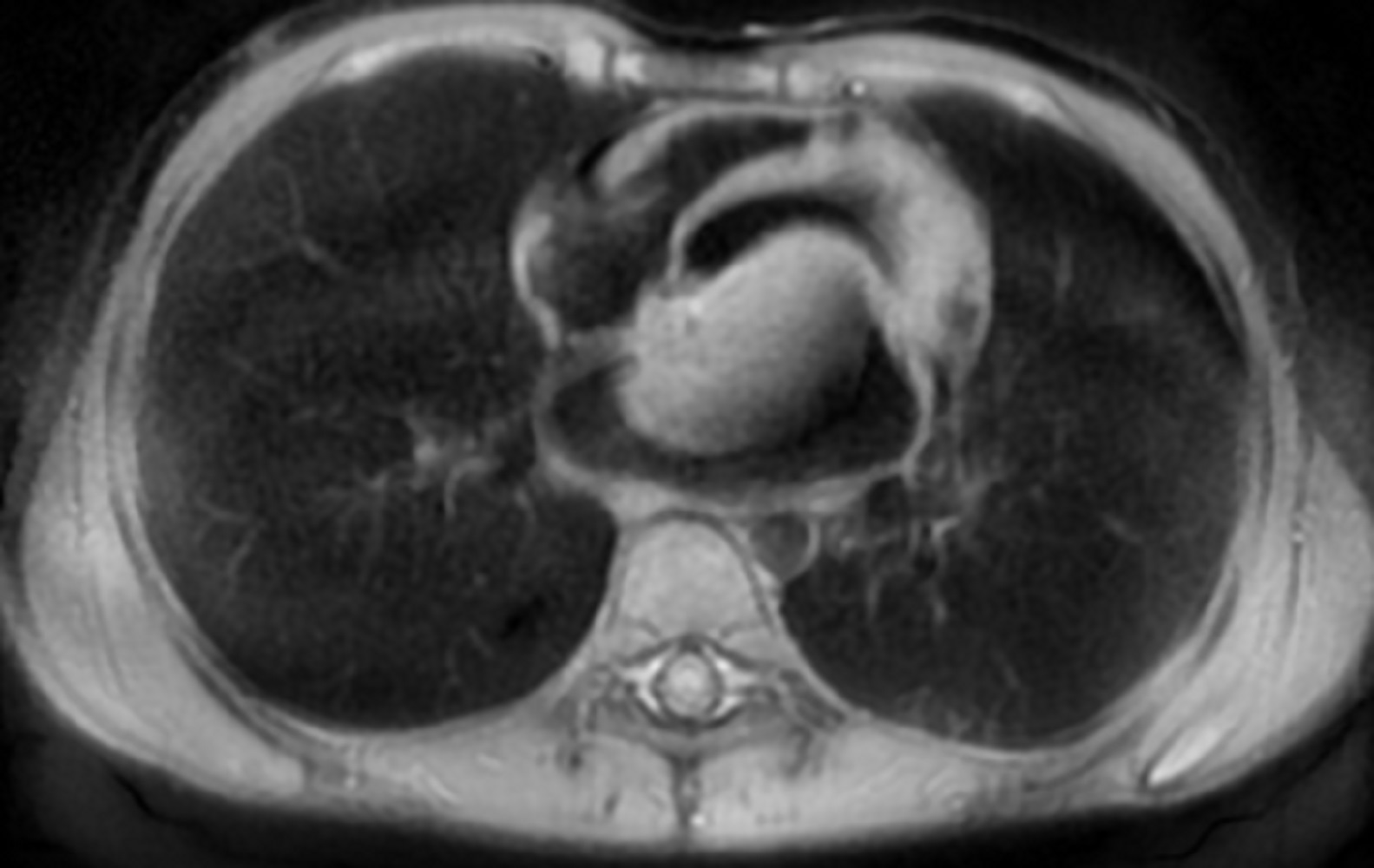
Figure 2. T1 double inversion recovery sequence with fat saturation showing a large hyperintense mass in left atrium.
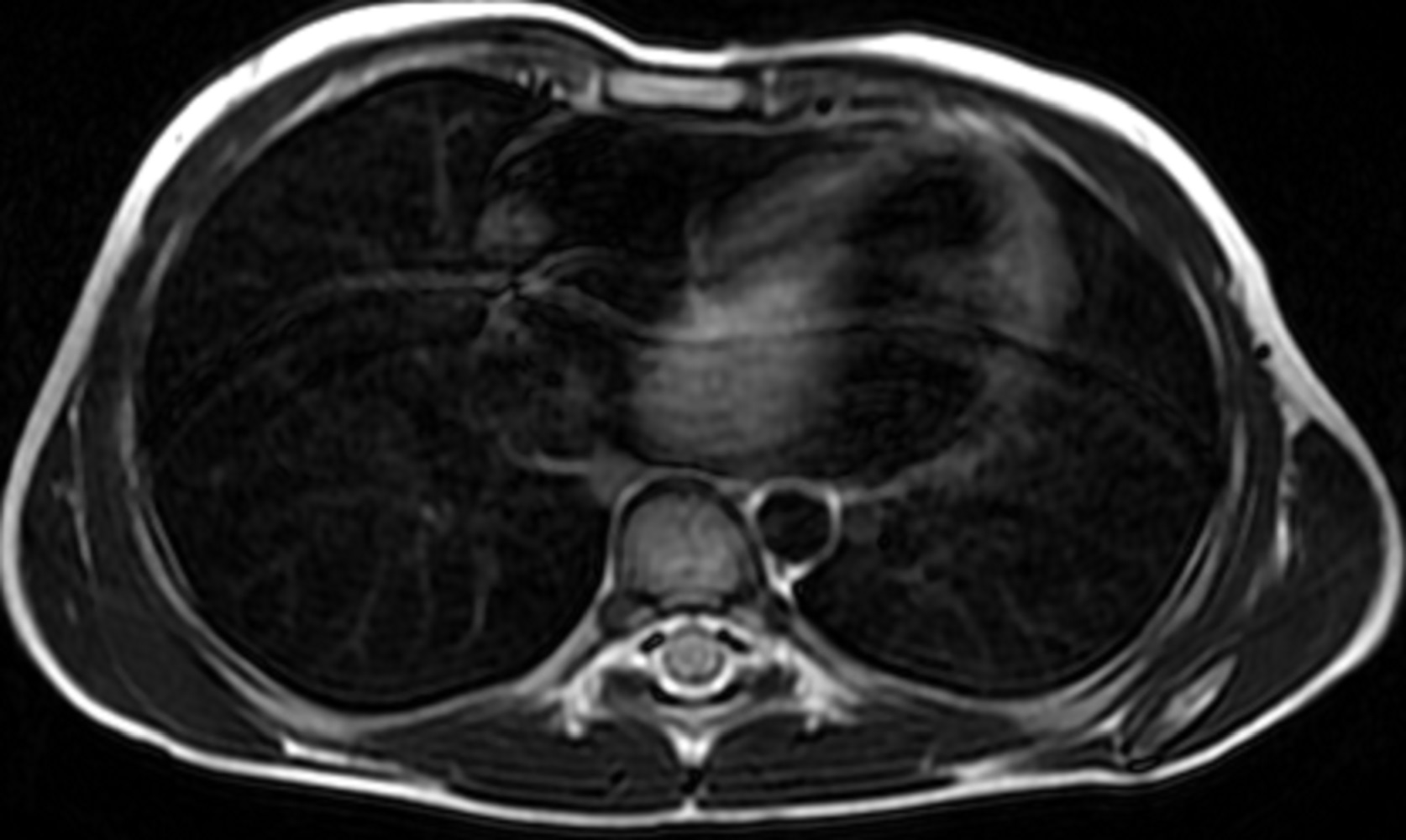
Figure 3. T2 double inversion recovery sequence showing hyperintense large mass in the left atrium
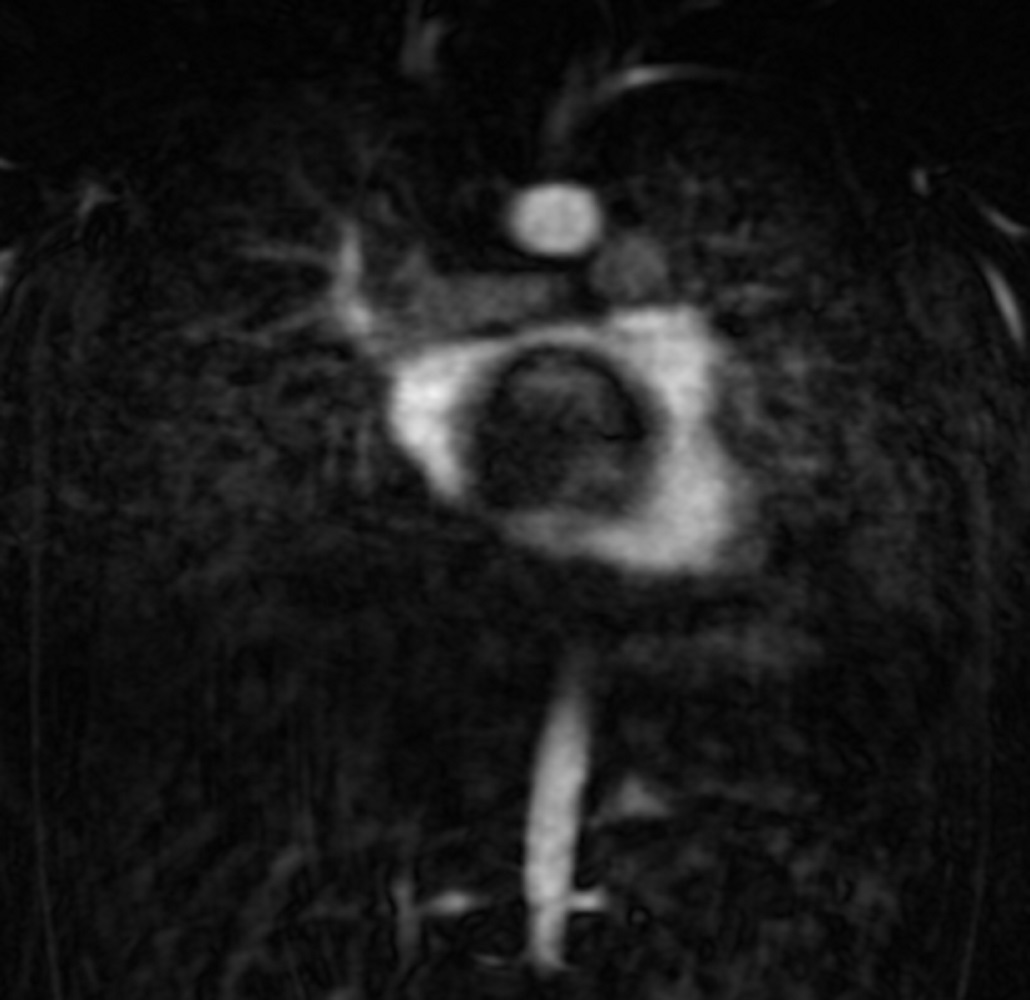
Figure 4. Coronal first pass angiogram showing no mass enhancement
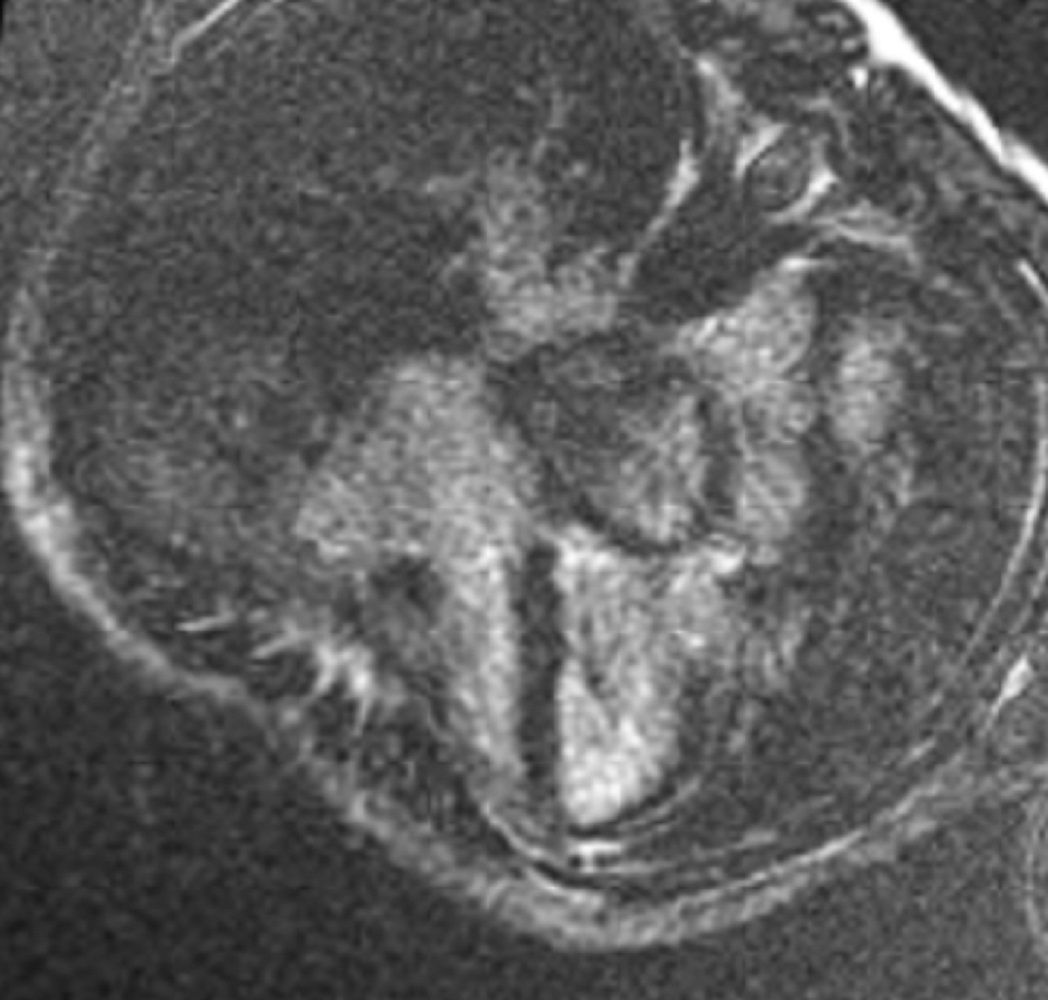
Figure 5. Myocardial delayed enhancement four chamber view showing variable intensity of the mass, which could be an India ink artifact.
Movie 4. Axial cine SSFP showing a large hypointense mass in left atrium likely attached to interatrial septum at the superior edge of the fossa ovalis close to the pulmonary vein entrance
Movie 5. Cine SSFP four chamber view showing large variably hypointense mass bulging into the left ventricle during diastole causing dynamic mitral stenosis
Conclusion
Intra-operatively, after being placed on cardiopulmonary bypass, the left atrial tumor was resected through the right atrium by excising the fossa ovalis. The tumor measured approximately 6cm x 4cm (Figure 6&7) with clear demarcation of the stalk’s attachment to the septum secundum and apex of the fossa ovalis between the pulmonary veins. An atrial septum repair with a pericardial patch was completed. Pathology confirmed the diagnosis of a left atrial myxoma. The patient had an insignificant post-operative course and was doing well in follow-up at one year.
This case demonstrates the importance of CMR in the diagnosis and management of cardiac tumors in children especially in the rare occurrence of a solitary tumor. In our case, the cardiac tumor was easily seen on echocardiography, but the actual diagnosis could only be suspected. CMR findings characterized the tumor as an atrial myxoma and although CMR has been shown to be highly accurate at differentiating between benign and malignant lesions, pathology remains the diagnostic gold standard (2). Most importantly, CMR helped to pinpoint the location of the stalk, which was instrumental for complete resection of the tumor without collateral damage to the pulmonary veins or mitral valve.
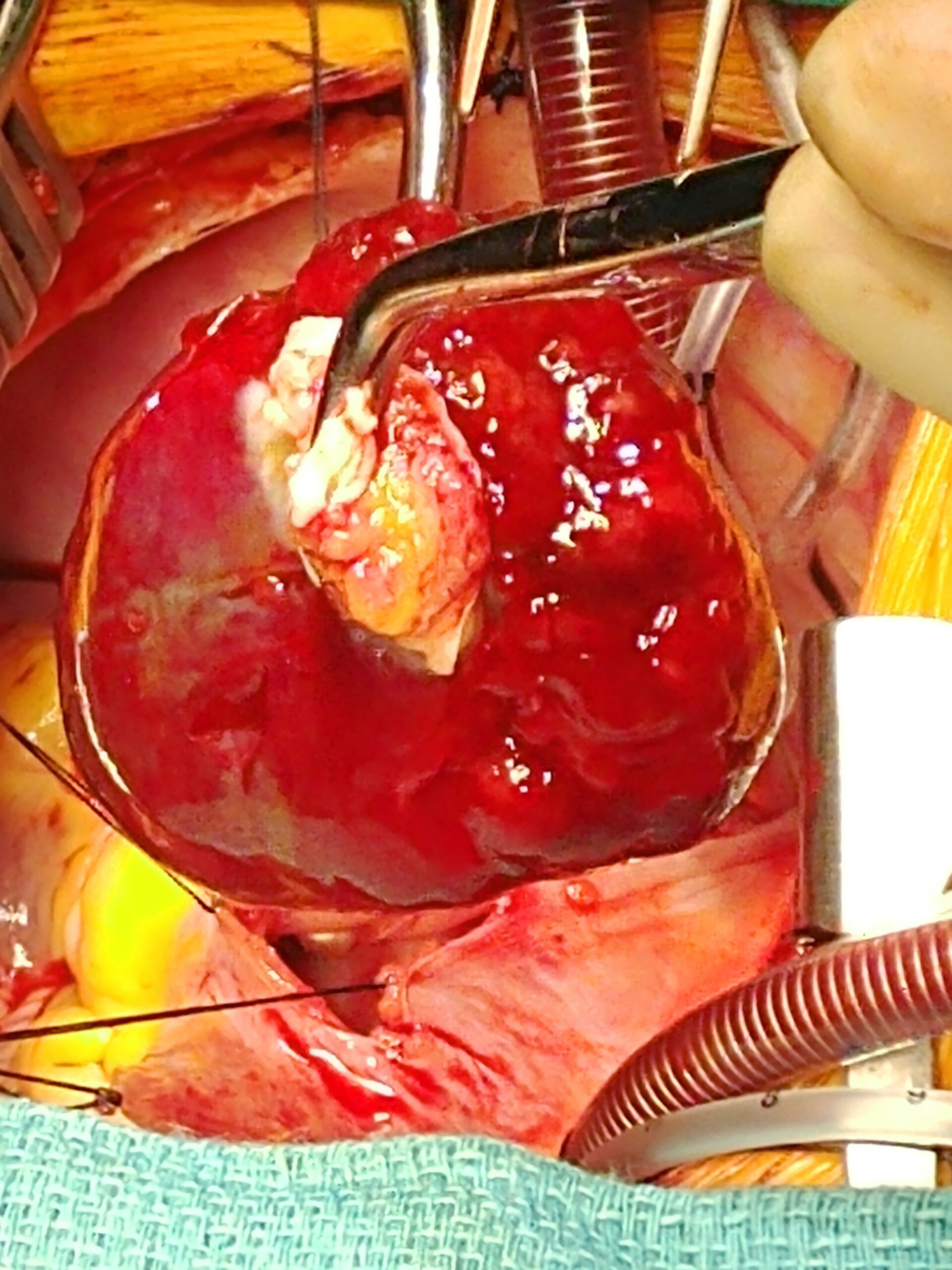
Figure 6: Removal of myxoma by left atrial stalk
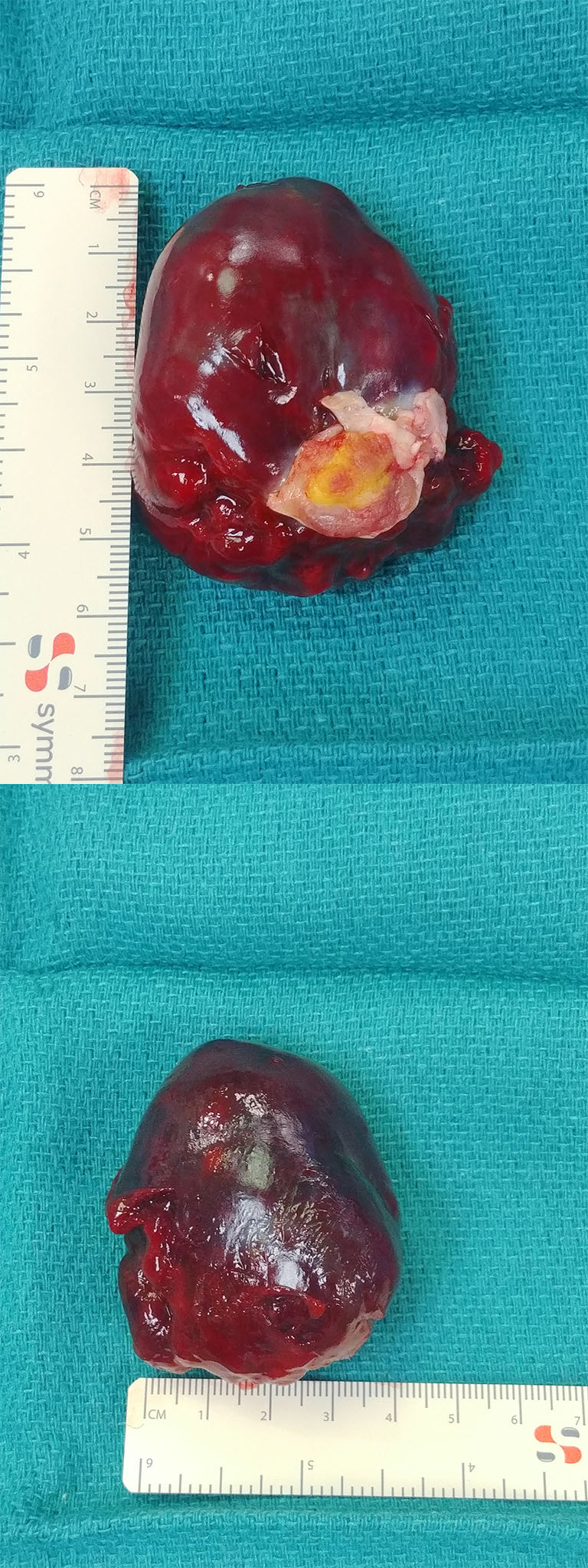
Figure 7: Resected tumor measuring approximately 6cm x 4cm
Perspective
Cardiac tumors in children have a reported incidence of 0.027-0.08%, most of which are benign (1). A differential for cardiac tumors may include: myxoma, fibroma, rhabdomyoma, malignancy, thrombus, teratoma, lipoma, and vascular tumors. CMR, along with the clinical correlation, are helpful tools when predicting the diagnosis of solid cardiac tumors. Location and different signal characteristics on commonly used MR techniques of SSFP, T1&T2 Turbo Spin Echo, myocardial perfusion, and late enhancement imaging are highly predictive of particular tumors. For example, a thrombus is often mural or intraluminal with hypointensity on all sequences (1).
Cardiac myxomas are often diagnosed in adults and presentation in children is very rare, generally presenting as part of a genetic syndrome (3–6). Myxomas develop most commonly in the left atrium (60%), followed by the right atrium (28%) and rarely in the ventricles (7). They typically arise near the fossa ovalis and more rarely from the atrial free wall close to the pulmonary veins or from the atrioventricular valves (7).
The uniqueness of this case stems from the patient’s young age and relatively benign presentation. Large myxomas, like the one in this patient, often present with systemic embolization, mitral valve obstruction or constitutional symptoms (5,8). An important consideration when children present with a cardiac myxoma is to screen for possible genetic causes i.e. Carney complex (9). Carney complex is a rare autosomal dominant syndrome associated with pigmented lesions of the skin and mucosa as well as various types of myxomas and endocrine tumors (8). The syndrome is due to mutations of the PRKAR1A gene in more than 70% of cases (8). Other genetic causes are not well understood. Recurrence of the tumor is common in multiple and familial cases (5). In this case, genetic testing revealed no syndrome as a cause for the myxoma.
Click here to review the case on CloudCMR.
References:
4. Reynen K. Cardiac myxomas. N Engl J Med. 1995;333(24):1610–7.
8. Correa R, Salpea P, Stratakis CA. Carney complex: an update. Eur J Endocrinol. 2015;173(4):M85–97.
Case prepared by:
Jason N. Johnson, MD MHS
Associate Editor, SCMR Case of the Week
Le Bonheur Children’s Hospital, University of Tennessee Health Science Center, St. Jude Children’s Research Hospital