



Campbell MJ, Darty S, Kim HW
Duke University, Duke Cardiovascular Magnetic Resonance Center, Durham, NC, USA
Case Published in the Journal of Cardiovascular Magnetic Resonance: Click here for the link
Click here for PubMed Reference to Cite this Case
Clinical History:
A 28 year old asymptomatic male with a history of Klippel-Feil syndrome was referred for a transthoracic echocardiogram because of his history of a genetic condition. The echocardiogram revealed an enlarged right atrium and ventricle and possible left to right atrial level shunt.
The patient was diagnosed with Klippel-Feil syndrome at 16 years of age when he was found to have multiple vertebral anomalies (fusion of C2-3, C7-T1, T2-3) as part of an evaluation for scoliosis. He subsequently had an abdominal ultrasound which revealed an absent left kidney.
CMR Findings:
A CMR scan was performed on a 1.5T Siemens Sola. The CMR revealed a secundum atrial septal defect which measured 1.5 x 1.3 cm and had a Qp/Qs of 1.4 measured by phase contrast (Movie 1-2). There was moderate to severe right atrial enlargement and a mild to moderately dilated right ventricle (RVEDV 245 ml, RVEDVi 123 ml/m2, RVESV 95 ml, RVESVi 48 ml/m2) with normal systolic function (RVEF=61%) (Movie 3).
There was an incidental finding of an aortic arch abnormality. The aortic arch was right sided and took a retroesophageal course to descend on the left side of the thorax. The first head and neck vessel was the left common carotid artery followed, in order, by the right common carotid, right subclavian, and left subclavian (Movie 4-6).
Movie 1: Long axis axial cine image demonstrating an enlarged right atrium and ventricle with a secundum atial septal defect with left to right shunt.
Movie 2: Coronal velocity encoded image demonstrating a moderate secundum atrial septal defect measuring 1.5 x 1.3 cm.
Movie 3: Short axis cine image at the mid-ventricular level illustrating mild to moderate right ventricular dilation with normal systolic function.

Movie 4: ECG gated contrast angiogram in a coronal plane illustrating right sided aortic arch with a left descending aorta and aberrant left subclavian artery.
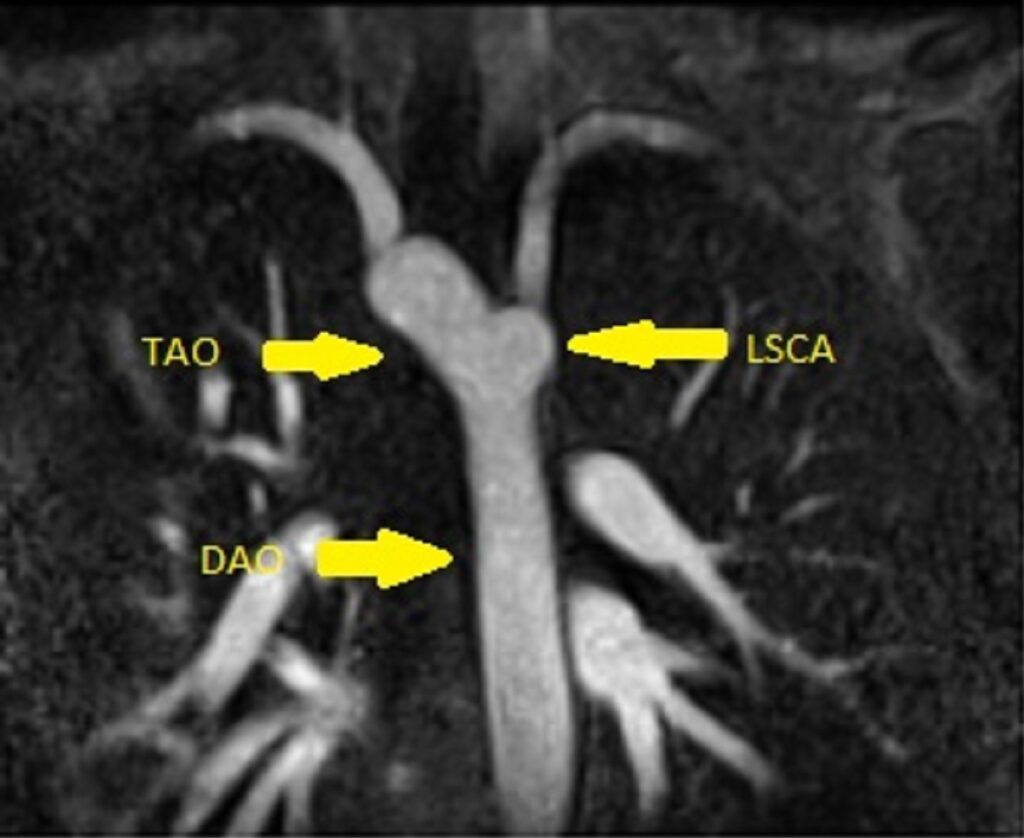
Image 1. Still frame angiogram in a coronal plane illustrating right sided transverse aortic arch (TAO) with a left descending aorta (DAO) and aberrant left subclavian artery (LSCA).

Movie 5: ECG gated contrast angiogram in an axial plane illustrating right sided aortic arch with a left descending aorta and aberrant left subclavian artery.
Image 2. Still frame angiogram in an axial plane illustrating right sided transverse aortic arch (TAO) with a left descending aorta (DAO) and aberrant left subclavian artery (LSCA). AAO = Ascending aorta
Movie 6: 3D reconstruction of aortic arch illustrating right sided aortic arch with a left descending aorta and aberrant left subclavian artery.
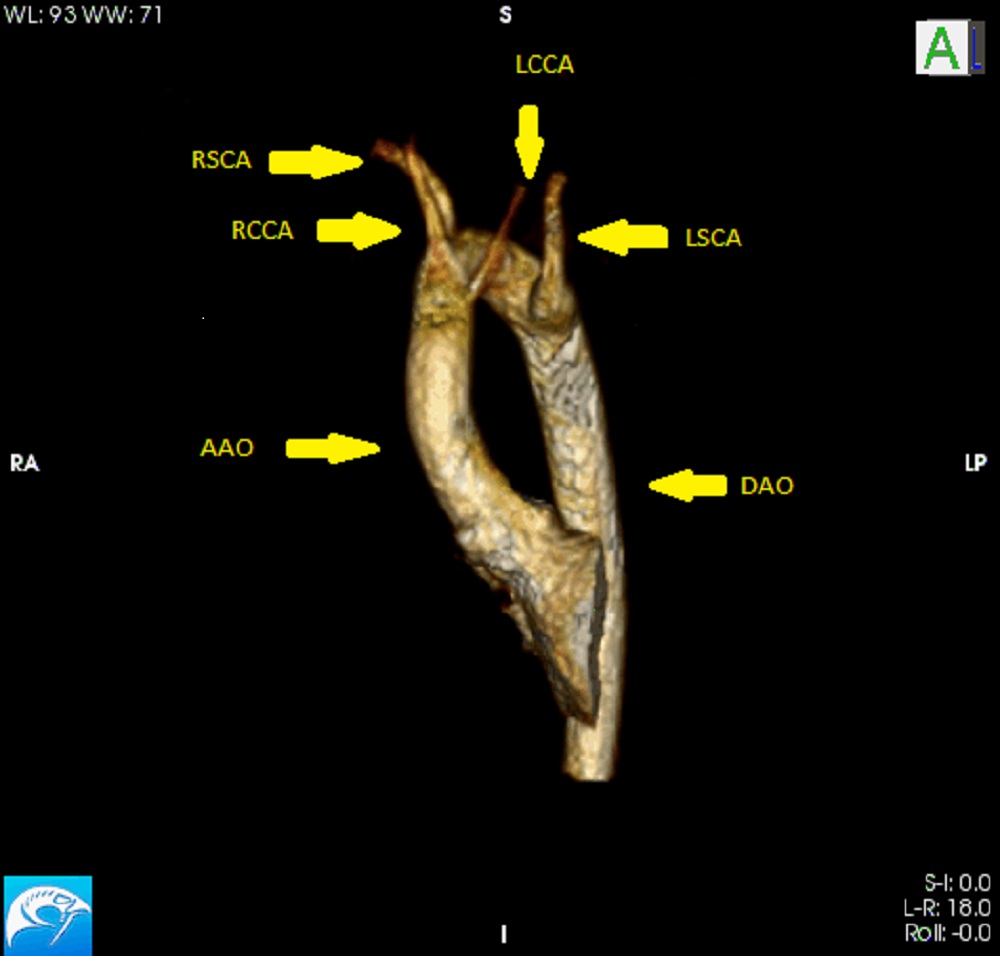
Image 3. Still frame 3D reconstruction of aortic arch illustrating right sided aortic arch with a left descending aorta (DAO) and aberrant left subclavian artery (LSCA). AAO = Ascending aorta; LCCA = Left common carotid artery; RCCA = Right common carotid artery; RSCA = Right subclavian artery
Conclusion:
This aortic arch anatomy is consistent with a diagnosis of a right sided aortic arch with a left descending aorta and a left arterial ductus arteriosus, also known as a right aortic arch with a retroesophageal segment or circumflex retroesophageal right aortic arch (1). There is also a secundum atrial septal defect. The patient is being evaluated for percutaneous closure of the secundum atrial septal defect. Division of the vascular ring is not being considered because of the patient’s asymptomatic status.
Perspective:
Klippel-Feil syndrome is a musculoskeletal condition defined by the fusion of at least 2 vertebrae in the neck (2). The syndrome is associated with a short neck, low hairline, and restricted mobility of the upper spine (2). It can also be associated with congenital heart defects, most commonly septal defects, as in this patient (3). Arch anomalies such as coarctation of the aorta and a right-sided aortic arch have been previously described (3,4). Rare reports of abnormalities of the head and neck arteries have also been described (5,6).
This case is consistent with a right-sided aortic arch as the transverse arch crosses over the right bronchus. A right sided aortic arch with a left descending aorta is a rare aortic arch abnormality occurring in <10% of right sided aortic arches (7). This diagnosis is associated with other congenital heart disease in 50% of patients (7). With this arch anatomy, the aortic arch crosses the midline at the level of the T4-5 vertebrae (1). The first branch can be the innominate artery or the left common carotid with an aberrant left subclavian, as in this case (1). From an embryonic standpoint, the anatomy reported here is caused by dissolution of the embryonic fourth aortic arch causing the left seventh intersegmental artery to originate from the proximal descending aorta via the left dorsal aorta (8). Persistence of the left sixth aortic arch results in a left sided ductus arteriosus (8). This anatomy is consistent with a vascular ring. This differential diagnosis includes a double aortic arch with an atretic left arch (1). These two diagnosis cannot be differentiated without surgical visualization; however, this case was unlikely a double aortic arch because of the absence of a remnant of the left atretic arch from the descending aorta. CMR was critical for the diagnosis of the aortic arch abnormality in this patient.
Click here to view the entire study via CloudCMR.
References:
- Weinberg PM (2001). Aortic arch anomalies. In Allen HD, Moss and Adams’ Heart Disease in Infants, Children, and Adolescents. 717-726. Lippincott Williams and Wilkins. Philadelphia, PA.
- Frikha R. Klippel-Feil syndrome: a review of the literature. Clin Dysmorphol. 2020 Jan;29(1):35-37.
- Hensinger RN, Lang JE, MacEwen GD. Klippel Feil syndrome: a constellation of associated anomalies. J Bone Joint Surg Am. 1974 Sep;56(6):1246-53.
- Falk RH, Mackinnon J. Klippel-Feil syndrome associated with aortic coarctation. Br Heart J. 1976 Nov;38(11):1220-1.
- Kandemirli SG. Intrathoracic bifurcation of the left common carotid artery associated with rib fusion and Klippel-Feil syndrome. Surg Radiol Anat. 2020 Apr;42(4): 411-15.
- Mubarak AI, Morani AC. Anomalous vertebral arteries in Klippel-Feil syndrome with occipitalized atlas: CT angiography. Radiol Case Rep. 2018 Feb 22;13(2):434-6.
- Hastreiter AR, D’Cruz IA, Cantez T, Namin EP, Licata R. Right-sided aorta. I. Occurrence of right sided aortic arch in various types of congenital heart disease. II. Tight aortic arch, right descending aorta, and associated anomalies, Br Heart Journal. 1966:28. 722-739.
- Ezon DS, Penny DJ. (2016). Aortic arch and vascular anomalies. In Allen HD, Moss and Adams’ Heart Disease in Infants, Children, and Adolescents. 850-853. Wolters Kluwer. Philadelphia, PA.
Case prepared by:
Jason N. Johnson, MD MHS
Associate Editor, SCMR Case of the Week
Le Bonheur Children’s Hospital, University of Tennessee Health Science Center, St. Jude Children’s Research Hospital

