



Jason L. Williams, MD
Nationwide Children’s Hospital, Columbus, Ohio
M. Jay Campbell, MD
Duke University Medical Center, Durham, NC
Case Published in the Journal of Cardiovascular Magnetic Resonance: Click here for the link
Click here for PubMed Reference to Cite this Case
Clinical History: A 14-year-old male presented to a pediatric cardiologist following referral for a new murmur heard on sports physical examination and for cardiac evaluation of connective tissue disease due to concern for Marfanoid features. His cardiac history was unremarkable, and there was no family history of connective tissue disease or sudden unexplained death. His medical history was notable for two years of progressive pectus carinatum. He was followed by orthopedics and was recommended for treatment with a brace. Physical exam was notable for a harsh grade III/VI systolic murmur best heard at the mid-left sternal border. Physical exam findings were also notable for a superiorly positioned pectus excavatum and an inferiorly positioned asymmetric pectus carinatum. A positive wrist sign and pes planus were noted on exam. Notably absent were hindfoot deformity, thumb sign, and reduced elbow extension. A transthoracic echocardiogram was performed, which demonstrated dynamic compression of the right ventricular outflow tract with flow acceleration starting in the sub-valvar region and extending throughout the pulmonary trunk by Doppler assessment. The maximum velocity through the right ventricular outflow tract was 2.0-2.5 m/sec. The mitral and aortic valves were normal.
CMR Findings: A CMR (cardiac magnetic resonance) scan was performed on a 3T Siemens Sola. The CMR scan revealed a prominent pectus carinatum with chest wall asymmetry (prominence of the right chest) resulting in extrinsic compression of the right ventricular outflow tract and mild sub-pulmonary stenosis. The compression and narrowed infundibulum were demonstrated in multiple imaging planes.
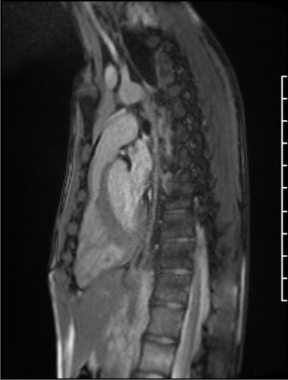
Figure 1: Sagittal projection demonstrating mild subvalvar pulmonary stenosis seen in the setting of a pectus deformity

Movie 1: Sagittal cine image demonstrating subvalvar narrowing

Movie 2: RVOT inplane flow demonstrating evidence of subvalvar obstruction.
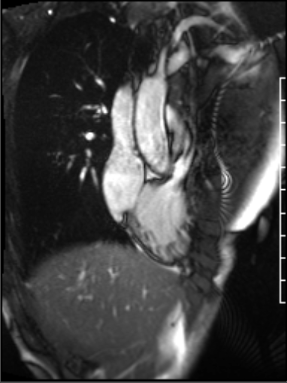
Figure 2: Mild subvalvar pulmonary stenosis demonstrated from a right ventricular long axis projection
The peak velocity was 245 cm/s. The AP diameter of the chest was noted to be significantly narrowed in the axial plane (Movie 3). The mitral and aortic valves were normal.
Movie 3: Significant subvalvar narrowing seen from an axial projection
Conclusion: The progression of the patient’s pectus carinatum and chest wall asymmetry during adolescence caused external compression of his right ventricular outflow tract, creating a functionally hypoplastic infundibulum with mild sub-pulmonary stenosis. Based on his comprehensive cardiac evaluation, he did not meet clinical criteria for Marfan Syndrome.
Perspective: Pectus excavatum and pectus carinatum are common anterior chest well deformities in children1,2. Pectus excavatum, the most common chest wall deformity, is defined as intrusion of the anterior chest wall into the thoracic cavity, which progresses as children age into adolescence 1,3. These deformities can be seen in patients with connective tissue disorders, such as Marfan Syndrome and Noonan Syndrome2.
CMR is a newer imaging modality used to diagnose pectus deformities and evaluate the degree of deformity in pre-surgical planning4. Patients can be asymptomatic; however, in one large adult cohort, 80% of patients had cardiac compression documented with symptoms of chest pain, dyspnea, palpitations, or exercise limitations5. Syncope has also been reported with a patient with severe pectus excavatum with compression of the right ventricle and left atrium in the anterior-posterior plane by CMR6.
CMR in recent years has provided dynamic assessment of cardiac structure and function during the respiratory cycle with exaggerated septal excursion and increased left ventricular eccentricity seen during the inspiratory phase 1,7. CMR also allows for a more comprehensive assessment of the effect of the pectus deformity on right ventricular dimensions and systolic function, as ultrasound has been shown to be discrepant when evaluating ventricular function1,8. Our patient was found to have normal right ventricular function by both modalities, despite a reduced effective right ventricular outflow tract.
CMR is a useful modality to evaluate the dynamic effects of pectus deformities on cardiac anatomy and function, and should be considered in a patient with a new murmur and pectus deformity.
Click here to view the case on CloudCMR: https://www.cloudcmr.com/8257-1973-4558-0103/
References:
Case prepared by:
Robert D. Tunks, MD
Associate Editor, SCMR Case of the Week