



Case from: Lamia Ait-Ali*§,MD, PhD, Bruno Murzi†, MD, MD, Pierluigi Festa§ ‡, MD
Institute: *Institute of Clinical Physiology, CNR, Massa-Pisa, Italy, § Pediatric Cardiology and GUCH unit, †Pediatric cardiac surgery, Heart hospital, Fondazione G. Monasterio-CNR, Regione Toscana, Massa, Italy. ‡ MRI Laboratory Fondazione G. Monasterio-CNR, Regione Toscana Pisa, Italy
Clinical history:
A symptomatic 50 year old woman previously diagnosed as congenitally corrected transposition of great arteries (L-TGA) was referred to our department. She was overweight and complained shortness of breath and palpitations.
Basal echocardiogram showed a situs solitus, levocardia, a small restrictive ventricular septal defect (VSD), associated to a mild sub-pulmonary stenosis and a severe sub-aortic tunnel –like stenosis with the aorta lying anteriorly and to the left of the pulmonary artery and finally two hypertrophied ventricles; however because of a bad acoustic window, the AV valve and ventricles morphology were not well identified. She was scheduled for Cardiac Magnetic Resonance (CMR) evaluation.
CMR Finding:
At CMR the following features were found: -the left side sided AV valve was bileaflet , therefore consistent with a mitral valve (Fig. 1; movie 1,2) and a morphological tricuspid valve was identified on the right side (atrio-ventricular concordance)
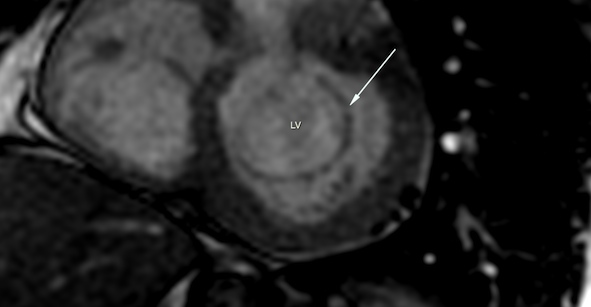
Figure 1

Movie 1

Fig 1: Still image and cine SSFP short axis ventricle (movie 1), 4 chamber view (movie 2): typical mitral valve (white arrow) connected to a posterior left ventricle. LA: left atrium; LV: Left ventricle.
-a sub-pulmonary VSD (Fig. 2) leading to a left-to-right shunt with QP/QS evaluated
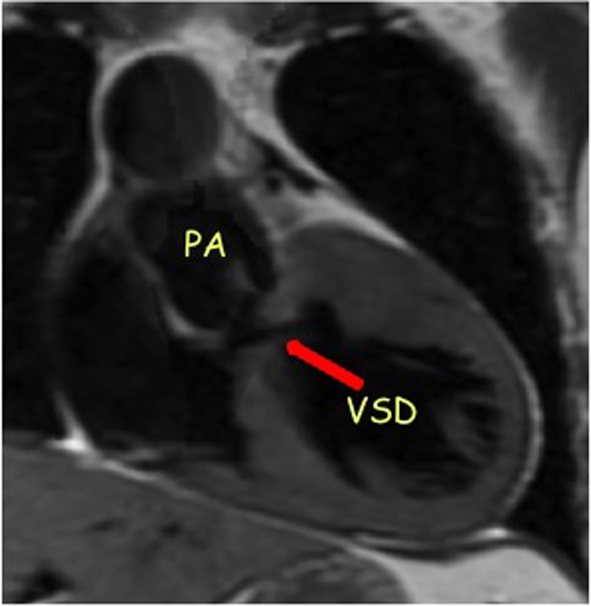
Fig 2: Black blood MR of right ventricle outflow tract showing a sub-pulmonary ventricular septal defect
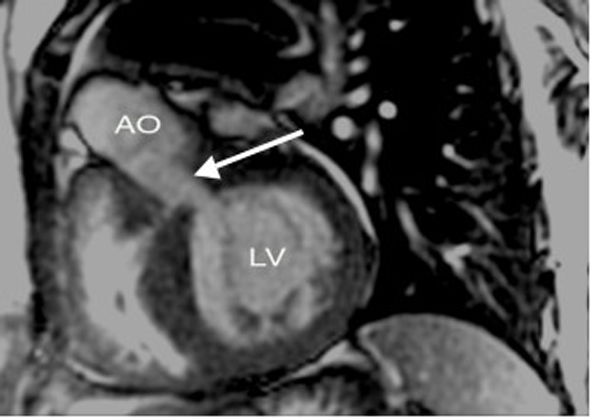

Fig 3, movie 3: Cine SSFP showing anterior aorta arising form the posterior LV through a stenotic fibromuscular tunnel (white arrow)
AO: aorta; LV: Left ventricle.
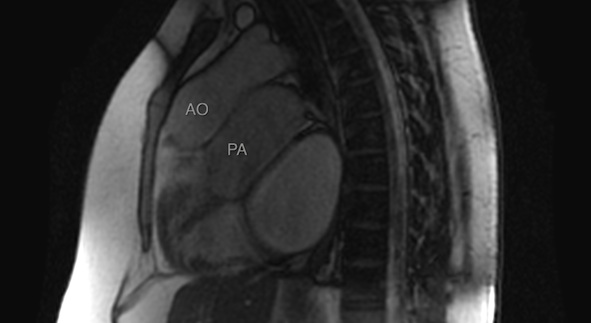
Fig 4, movie 4: Sagittal Cine SSFP showing anterior aorta arising form the posterior LV and a posterior pulmonary artery arising from the anterior RV
AO: aorta; LA: left atrium; LV: left ventricle; PA: pulmonary artery.
Movie 5: Axial stack showing the relations of the ventricles to the corresponding great vessels.
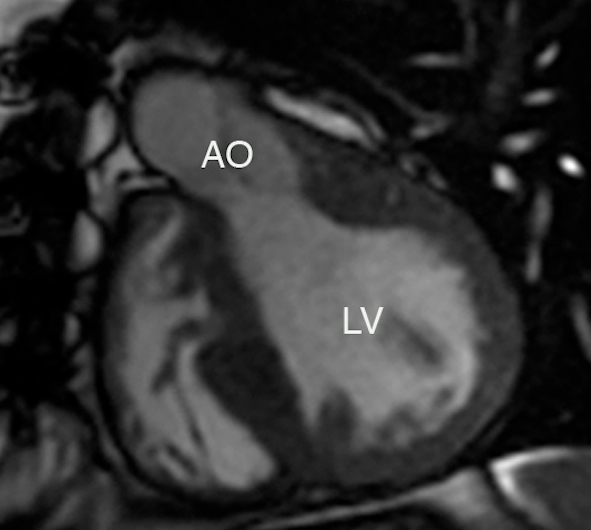
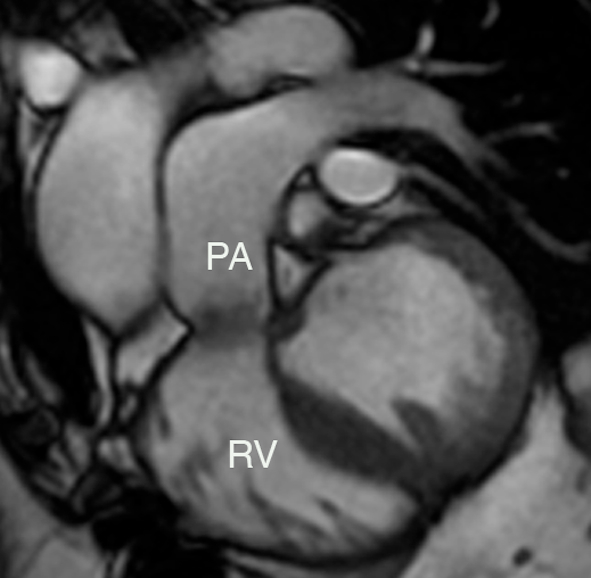
Fig 6: Post operative CMR
A) Cine SSFP left outflow tract
B) Cine SSFP right outflow tract
AO: aorta; LV: Left ventricle; PA: pulmonary artery: RV: right ventricle.
Perspective: CMR was critical to obtain the correct diagnosis of ACMGA, restrictive VSD, subaortic and subpulmonary stenosis. ACMGA is a very rare form of congenital heart disease in which the great arteries arise above the anatomically correct ventricles but are abnormally related to the ventricles and to each other [1,2]. Subaortic stenosis occurs in about 15% of ACMGA [3]. ACMGA is frequently misdiagnosed as congenitally corrected transposition (L-TGA)[4,5] however because of the technical problem of the ventricular septal defect closure to avoid the conduction pathway, they must be differentiated precisely [6]. CMR should be the preferred technique in this setting because it is radiation-free, has a high anatomic definition and overcomes some of the limitations of ultrasound mainly in adult patients.
References:
1. Van Praagh R, Durnin RE, Jockin H, Wagner HR, Korns M, Garabedian H, Ando M, Calder L (1975) Anatomically corrected malposition of the great arteries. Circulation 1975;51:20–31.
2. Van Praagh R. The story of anatomically corrected malposition of the great arteries. Chest. 1976;69:2–4. 7. 3.
3. Bernasconi A, Cavalle-Garrido T, Perrin DG, Anderson RH: What s anatomically corrected malposition? Cardiol Young 2007;17:26-34.
4. Oku H, Shirotani H, Yokoyama T, Kawai J, Nishioka T, Noritake S et al. “Anatomically corrected malposition of the great arteries–case reports and a review.” Jpn Circ J. 1982;46:583-594.
5. Rittenhouse EA, Tenckhoff L, Kawabori I, Mansfield PB, Hall DG, Brown JW. Surgical repair of anatomically corrected malposition of the great arteries. Ann Thorac Surg.1986;42:220–8.
6. Anderson RH, Becker AE, Losekoot TG, Gerlis LM. Anatomically corrected malposition of great arteries. Br Heart J. 1975 Oct;37(10):993-1013.

