



Case from: Ahmed A. Kolkailah1,2 MB BCh, Leelakrishna Nallamshetty
3 MD, Siva K. Kumar2 MD, Tony Fattouch3 MD, Carlos A. Rojas3 MD
Institute: 1Ain Shams University Faculty of Medicine, Abbassia Square,
Cairo, Egypt; 2Tampa General Hospital, Tampa, FL; 3University of South Florida Morsani College of Medicine, Tampa, FL.
Clinical history:
A 64 year old male presented one year after cardiac transplant for routine follow up. A 2D transthoracic echocardiogram revealed a mobile, echogenic lesion along the inferior wall of the right atrium.
The lesion demonstrated by 2D transthoracic echocardiogram (see Figure 1 and Movie 1) prompted the need for further characterization by CMRI.
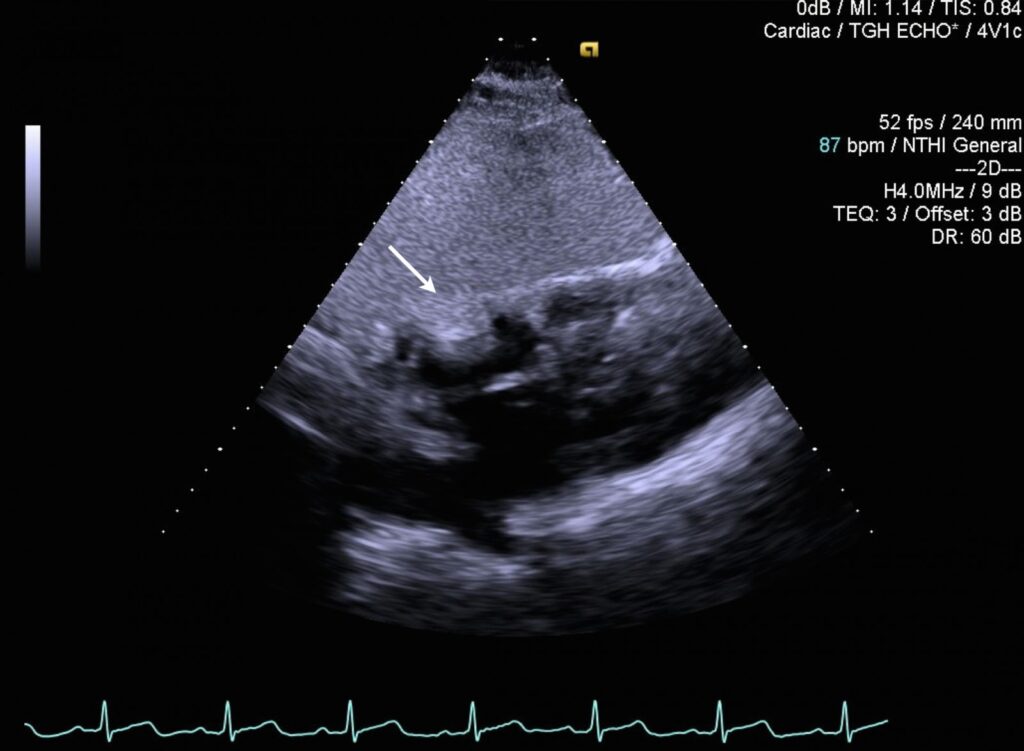
Figure 1: 2D Transthoracic echocardiogram in the subcostal 4-chamber projection demonstrates an echogenic lesion which appears to originate from the inferior wall of the right atrium and projects into the right atrium.
Movie 1.2D Transthoracic echocardiogram in the subcostal 4-chamber projection demonstrates an echogenic lesion which appears to originate from the inferior wall of the right atrium and projects into the right atrium.
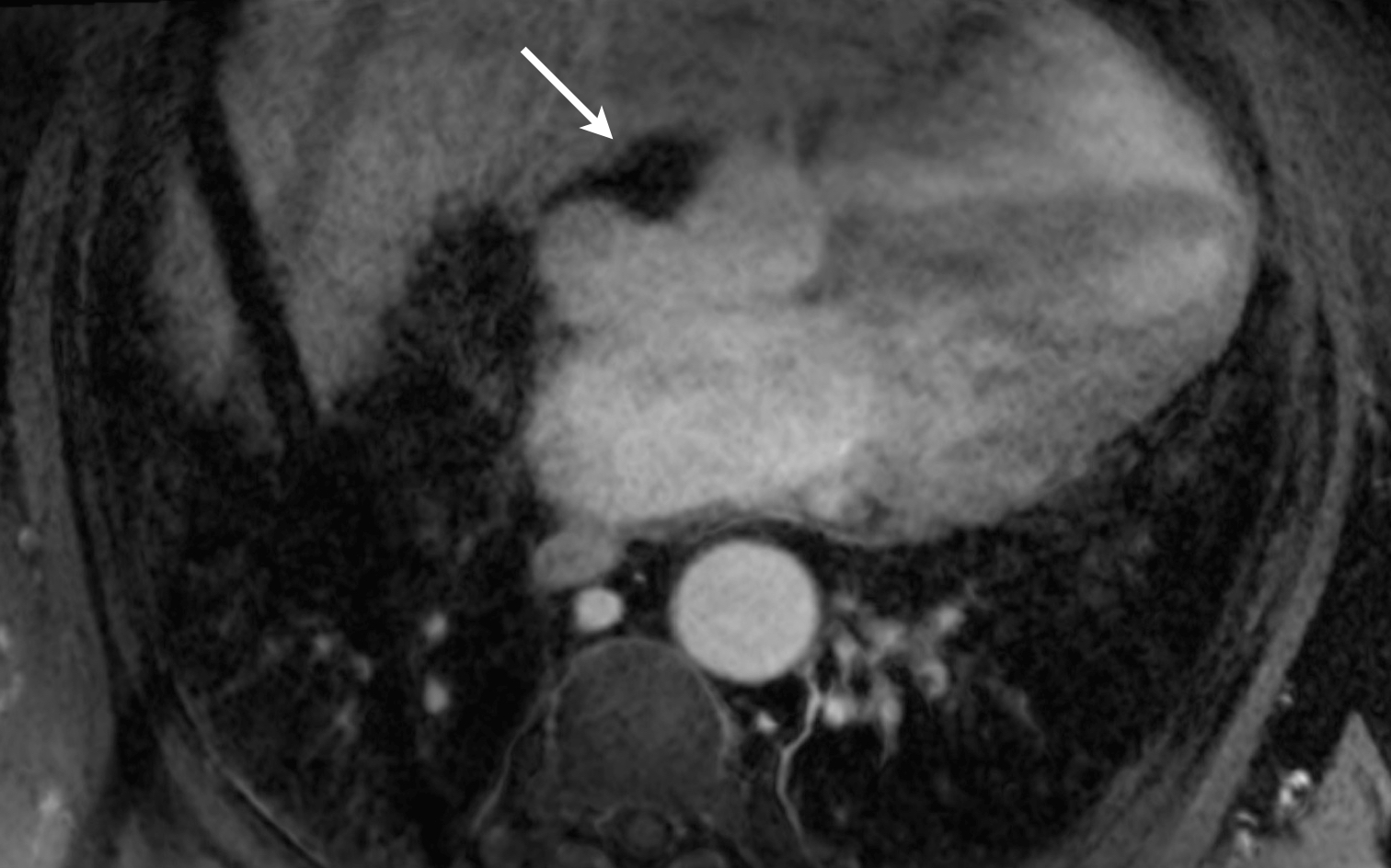
Figure 2: Fat suppressed 3D whole heart image of Cardiac MRI after contrast in the 4-chamber plane demonstrates a hypointense extracardiac lesion which invaginates the right atrium. The 3D whole heart sequence is an ECG gated, free breathing, respiratory navigated sequence on a 3T-MRI scanner (Verio, Siemens). Bolus tracking method was utilized with timing designed for peak opacification of the right ventricle. 0.2 mmol/kg of gadobenate dimeglumine. Imaging parameters were: TR/TE 549/1.34 ms, FOV (640×400), matrix 220×320, voxel size (1.3 mm). The isotropic image data set was reformatted offline.
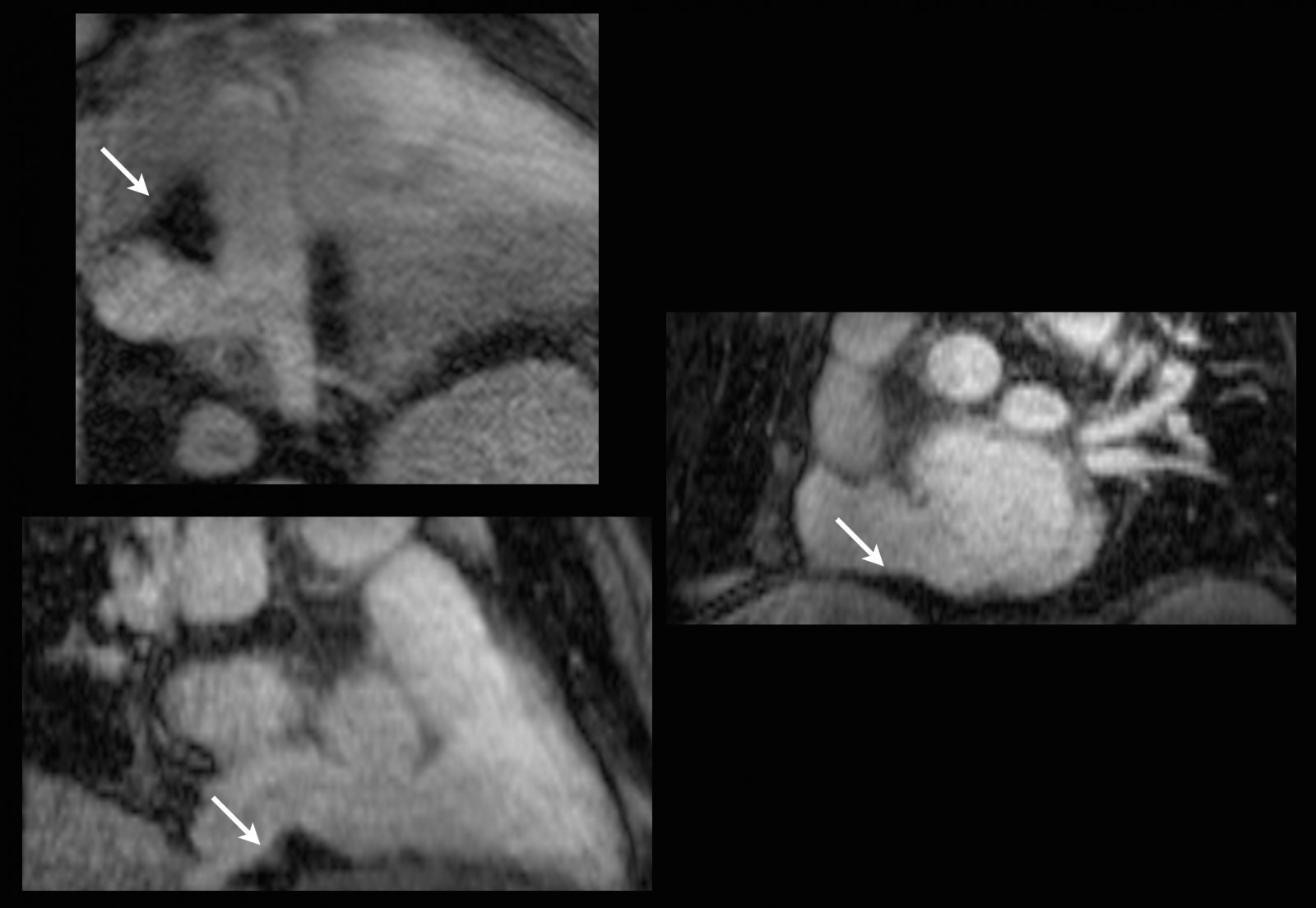
Figure 3: The multiplanar reformatted image demonstrates the lesion to be epicardial in origin rather than intracardiac.
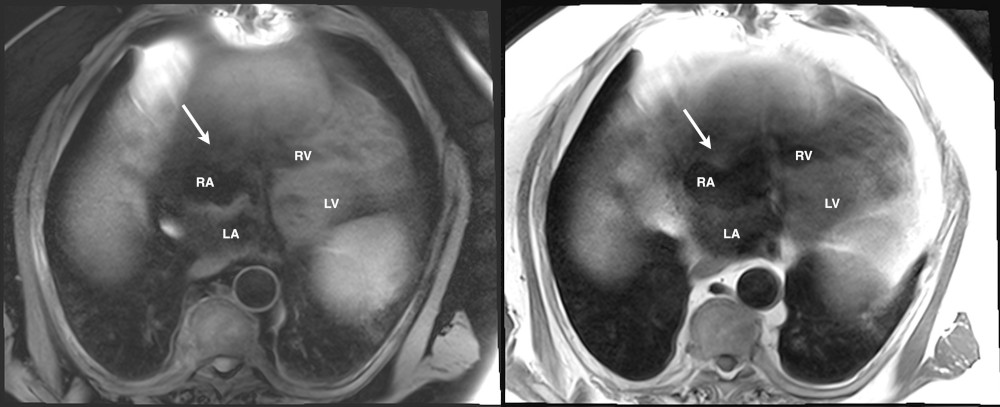
Figure 4. T1W with and without fat suppression, respectively.
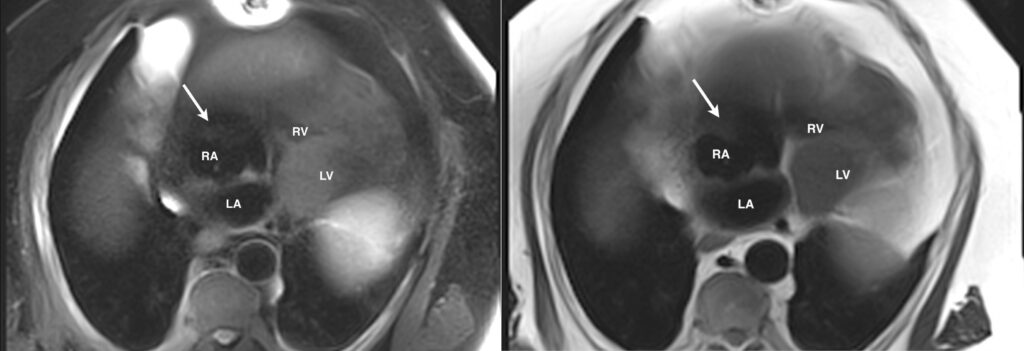
Figure 5. T2W with and without fat suppression, respectively.

Movie 2a.Balanced steady state free precession (bSSFP) oblique view demonstrating right atrial invagination by extra-cardiac mass.
Movie 2b. Balanced steady state free precession (bSSFP) 4-chamber view demonstrating right atrial invagination by extra-cardiac mass.
Movie 3.Gadolinium contrast enhanced first pass perfusion demonstrating no perfusion of the extra-cardiac mass.
Conclusion:
Our case describes an uncommon finding on echocardiography and stresses the importance of cross sectional imaging in the evaluation of cardiac masses. As a result of correctly diagnosing this lesion as extracardiac epicardial fat rather than a true intra-cardiac mass, management was significantly altered whereby the patient no longer required cardiac surgery.
Perspective:
The value of echocardiography for diagnosing cardiac and extracardiac masses has been well established dating back to 1951 when an atrial myxoma was first demonstrated utilizing ultrasonography as an imaging modality by Effert and Domanig.1
Since then, cardiac ultrasound has evolved enormously and is currently the first line imaging modality of choice for the evaluation of space-occupying lesions of the heart; it provides high quality, real-time images that are critical in the assessment of cardiac masses.2 It does, however, have its own limitations due to patient dependent factors such as body habitus and acoustic windows in addition to the skill/ability of technologist. Obesity and lung diseases are prevalent and result in suboptimal image quality.3 Furthermore, tissue characterization is somewhat limited with echocardiography.
Our case emphasizes the importance of using multi-modality imaging techniques in the workup of intra and extracardiac masses. It also sheds light on the critical role of cardiac magnetic resonance imaging as an adjunct to 2D echocardiography when unexpected findings are discovered. The inclusion of advanced cardiac imaging modalities will ensure accuracy in diagnosis and help appropriately direct patient clinical management.
References:

